This report describes the treatment of a 13-year-old girl with unerupted maxillary permanent canines. It illustrates how recognizing an unexpected problem influenced the decision-making process. Despite 6 months of closed-eruption traction, the left canine had not erupted. However, the neighboring teeth were intruded, suggesting a diagnosis of canine ankylosis. When the site was surgically reopened, the wire chain used for the orthodontic traction appeared to be osseointegrated. It was renewed, and traction was applied for another 16 months, and the tooth was successfully brought into the arch. Bone tissue passing through the chain might have prevented forced eruption. In young patients with unerupted maxillary permanent canines, failure of closed traction can be attributed to ankylosis, and this accounts for tooth extraction as the treatment of choice. However, this clinical report suggests that additional measures might be warranted before the definitive diagnosis of ankylosis can be made and the tooth extracted.
Impaction of the maxillary permanent canine has an estimated prevalence of 1.7% in the general population, but the incidence might be higher in those who have been referred to orthodontists. This might be explained by the tooth being deflected from its normal eruptive path and becoming either labially, centrally, or, more often, palatally impacted.
With an adequate clinical and radiographic diagnosis in the mixed dentition stage, palatally or centrally displaced maxillary permanent canines have been shown to frequently correct with early extraction of the deciduous canines, or concomitant extraction of the deciduous canines and first molars. This reduces the need for orthodontic appliances and also the incidence of resorption on the adjacent incisor roots, which might occur in nearly 50% of patients with ectopic canines.
If the diagnosis is made at a later stage (after 12-13 years of age), surgical exposure followed by traction of the tooth with orthodontic forces is often required. Failures to respond to direct orthodontic extrusive traction in the absence of any mechanical obstruction of the eruption pathway (caused by odontomas, odontogenic tumors, or supernumerary teeth) have been generally attributed to an unhealthy periodontal membrane (ie, tooth ankylosis).
The purpose of this clinical report was to describe an unexpected problem encountered during the treatment of an unerupted maxillary permanent canine, the recognition of which enabled a change in the diagnosis and, consequently, in the decision-making process, thus allowing a successful clinical outcome.
Case report
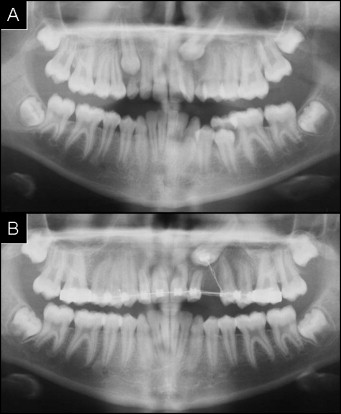
A 13-year-old girl was referred for orthodontic consultation. The clinical examination showed an Angle Class I occlusion with moderate mandibular anterior crowding and persistence of both the maxillary right and left deciduous canines ( Fig 1 ). The patient’s medical and dental histories were unremarkable, and no family history of maxillary canine impactions was reported. No maxillary permanent canine bulges could be palpated. There was distal-palatal rotation of the maxillary left lateral incisor, possibly due to a displaced permanent canine lying on its root ( Fig 1 ). Panoramic and periapical radiographs confirmed the presence of both unerupted maxillary permanent canines; the right canine was centrally located in a vertical position, and the left canine was palatally displaced and inclined mesially, high in the alveolar process, with its crown overlapping the root of the adjacent lateral incisor ( Fig 2 , A ).

The treatment plan consisting of a surgical-orthodontic approach was explained to the patient and her parents, and their informed consent was obtained.
The maxillary deciduous canines were extracted, both maxillary permanent canines were surgically exposed under local anesthesia, and an orthodontic buttonhole connected to a wire chain was bonded directly onto them. Initially, orthodontic traction was activated on the right canine only to prevent excessive vertical and anteroposterior anchorage loss on the maxillary permanent incisors. Furthermore, due to a relatively more feasible position, this tooth should have been brought into the arch in a shorter period of time compared with the left canine.
The tooth successfully erupted during 2 months of orthodontic traction, and a bracket was bonded on its buccal surface. Once fully aligned in the dental arch, greater anchorage had been obtained for orthodontic extrusive traction to be activated on the left side.
After 6 months of orthodontic traction by the closed-eruption approach, clinical and radiographic analysis showed no movement of the left permanent canine associated with an intrusive movement of the adjacent teeth ( Figs 2 , B , and 3 ), suggesting a diagnosis of ankylosis. A second surgery was thus scheduled to remove the unerupted tooth. At reentry, the canine showed mobility, and the direction of orthodontic traction was correct, but the wire chain appeared to be osseointegrated ( Fig 4 ).

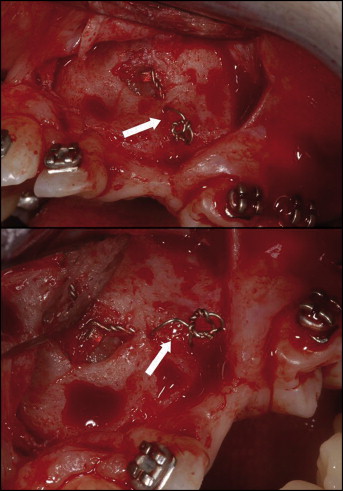
After that finding, the surgeon (G.D.) and the orthodontist (G.A.B.) decided not to extract the canine, but to renew the wire chain and reactivate the orthodontic traction on the left side. The evidence of initial tooth movement proved that the diagnosis of ankylosis was incorrect. For this reason, it was decided to continue the treatment, and, after a further 16 months of active orthodontic traction, the left permanent canine was successfully aligned in the dental arch ( Figs 5 and 6 ).



