Introduction
The regular collection of 3-dimensional (3D) imaging data is critical to the development and implementation of accurate predictive models of facial skeletal growth. However, repeated exposure to x-ray–based modalities such as cone-beam computed tomography has unknown risks that outweigh many potential benefits, especially in pediatric patients. One solution is to make inferences about the facial skeleton from external 3D surface morphology captured using safe nonionizing imaging modalities alone. However, the degree to which external 3D facial shape is an accurate proxy of skeletal morphology has not been previously quantified. As a first step in validating this approach, we tested the hypothesis that population-level variation in the 3D shape of the face and skeleton significantly covaries.
Methods
We retrospectively analyzed 3D surface and skeletal morphology from a previously collected cross-sectional cone-beam computed tomography database of nonsurgical orthodontics patients and used geometric morphometrics and multivariate statistics to test the hypothesis that shape variation in external face and internal skeleton covaries.
Results
External facial morphology is highly predictive of variation in internal skeletal shape ([ R v ] = 0.56, P <0.0001; partial least squares [PLS] 1-13 = 98.7% covariance, P <0.001) and asymmetry ( R v = 0.34, P <0.0001; PLS 1-5 = 90.2% covariance, P <0.001), whereas age-related ( r 2 = 0.84, P <0.001) and size-related ( r 2 = 0.67, P <0.001) shape variation was also highly correlated.
Conclusions
Surface morphology is a reliable source of proxy data for the characterization of skeletal shape variation and thus is particularly valuable in research designs where reducing potential long-term risks associated with radiologic imaging methods is warranted. We propose that longitudinal surface morphology from early childhood through late adolescence can be a valuable source of data that will facilitate the development of personalized craniodental and treatment plans and reduce exposure levels to as low as reasonably achievable.
Highlights
- •
We tested the relationship between variation in external facial morphology and internal skeletal shape.
- •
The face predicts variation in shape, asymmetry, and associated growth parameters of the skeleton.
- •
We speculate that standardized collection of facial surface morphology will contribute to generating accurate predictive models.
A goal of modern health care is to make individual patient care predictive, personalized, preventive, and participatory. In dentistry, the ability to accurately predict both how a patient’s craniofacial and mandibular skeleton will grow and the likelihood of any future need for clinical intervention would have a transformative effect on orthodontic and surgical practice. However, growth of the skeleton is both idiosyncratic and nonlinear, with individual structures differing in the timing, magnitude, rate, and duration of growth. As a consequence, cross-sectional estimates of age-related changes in shape and size provide only broad generalizations that are insufficient to predict a patient’s development. This critical limitation suggests that to realize personalized and predictive goals, longitudinal data on skeletal shape and size from the same subjects must be collected. Yet the long-term risks of repeatedly exposing pediatric patients to the ionizing modalities that image the skeleton are unknown and carry significant potential risks.
The relationship between the internal and external anatomies suggests a possible alternative to ionizing modalities for collecting longitudinal skeletal data. Notably, whereas the hard tissues are the principal locus of growth and surgical intervention, the soft tissues of the external face mirror this internal bony shape. This suggests that surface features alone—eg, those captured from nonionizing modalities such as 3-dimensional (3D) photography—may be sufficient to infer skeletal shape with high accuracy. However, despite the intuitive appeal of this hypothesis, it has not been directly tested. Moreover, the value of external surface morphology is only as good as the accuracy of its predictive relationship to internal skeletal shape.
We tested the hypothesis that variation in the shape of the face and skeleton significantly covaries using a retrospective analysis of a cone-beam computed tomography (CBCT) database. These data were originally collected during routine orthodontic assessment and patient care. They are appropriate to use here because surface and skeletal anatomies were captured simultaneously; this reduced the errors associated with registering different time points and facilitated the accurate comparison of covariation. If variation in surface morphology can be shown to significantly covary with internal skeletal shape variation, it would provide quantitative support for the collection of surface shapes and its use as a proxy for measures of skeletal shape. In contrast, a weak or nonsignificant relationship—eg, due to independent soft-tissue variation—would be problematic for the full use of resources in which external facial shape is the only regularly collected measurement. To address these alternatives, we used methods collectively known as landmark-based geometric morphometrics to quantify and test for covariation of shape and enable the direct visualization of the results of 3D objects.
Material and methods
This was a retrospective cross-sectional study with a population composed of skeletally normal patients (nonsurgical) previously assessed for orthodontic therapy at the University of California at San Francisco (N = 175; Table ). To be included in this study, subjects had to have a pretreatment CBCT scan obtained with consent from the institutional review board (University of California at San Francisco Committee on Human Research #10-00564; J.C.H., J.S.L.). All scans were generated between September 2010 and January 2011 and were originally collected for cephalometric assessments during standard orthodontic planning and treatment. This study included patients with dental crowding and an Angle Class I (ANB, −0.9°-2.5°), a tendency for Class II or Class II Division 2 (ANB, >2.5°), or a Class III (ANB, <−1°) malocclusion that was managed with orthodontic therapy only ( Table ). Patients were excluded from this study if they had a congenital anomaly or other known syndrome that affects craniofacial growth and development. Demographic information (age, sex) was linked to the CBCT data, with all personal identifiers removed (University of California at San Francisco Committee on Human Research #11-06996; N.M.Y.). The data set was stratified according to age (range, 7.5-57.6 years) and sex. Because growth of the facial skeleton is largely complete by early adulthood, all patients over 21 years of age were coded as 21.
| Age (y) | Angle Class (ANB) | Sex (n) | |||||
|---|---|---|---|---|---|---|---|
| I (−0.9°-2.5°) | II (>2.5°) | II Division 2 (>2.5°) | III (<−1°) | Female | Male | All | |
| 7-10 | 2 | 5 | 2 | 0 | 3 | 6 | 9 |
| 10-12 | 4 | 15 | 2 | 0 | 8 | 13 | 21 |
| 12-14 | 9 | 26 | 5 | 8 | 30 | 18 | 48 |
| 14-16 | 11 | 15 | 1 | 6 | 19 | 14 | 33 |
| 16-18 | 3 | 10 | 1 | 1 | 10 | 5 | 15 |
| 18-21 | 4 | 4 | 1 | 3 | 9 | 3 | 12 |
| >21 | 10 | 20 | 3 | 4 | 21 | 16 | 37 |
| Total | 43 | 95 | 15 | 22 | 100 | 75 | 175 |
| Mean | 1.30 | 5.35 | 5.77 | −3.64 | |||
| Minimum | −0.70 | 2.60 | 3.40 | −9.40 | |||
| Maximum | 2.50 | 10.60 | 9.70 | −1.00 | |||
| SD | 0.88 | 1.87 | 1.57 | 2.21 | |||
For the 3D data, first, a MercuRay CBCT scanner (Hitachi Medical, Tokyo, Japan) was used to generate images. CBCT uses a low-energy, fixed-anode tube, which produces a cone-shaped x-ray beam, a special image intensifier, and a solid-state sensor. The face was scanned only once, with a total radiation exposure estimated at about 200 μSv by the manufacturer. The subjects were seated upright as the x-ray tube and image acquisition screen revolved around their heads. Each subject was instructed to hold still, keep the teeth in occlusion, not swallow, and keep the tongue on the roof of the mouth and the head in a natural position. Scanner settings were 110 kVp and 10 mA, generating a total of 512 slices in a 10-second scan, with a 19 × 19 × 19-cm field of view. The images were reconstructed in CBWorks (version 2.1; Cyber Med, Seoul, Korea) and Avia (Hitachi Medical) and were saved in DICOM format. Second, for each subject, we reconstructed a 3D model in Amira (version 5.4; Visage Imaging, San Diego, Calif) using threshold values that best maximized either bone and tooth signals (eg, 0 ± 100) or external morphology (eg, −660 ± 30). Third, for each object, we applied homologous 3D landmarks (external face [midline, n = 9; bilateral, n = 10; total, 29], and internal facial skeleton and mandible [midline, n = 10; bilateral, n = 52; total, 114]) in Landmark Editor (version 3.6; University of California at Davis) ( Supplementary Fig S1 , Supplementary Table SI ). Fourth, potential sources of measurement error included (1) thresholding values, altering the reconstructed shape of 3D objects; and (2) location of landmarks, both within and between observers. We assessed these factors by thresholding and landmarking a subset of subjects (n = 30) on 3 occasions. Using the method of Starbuck et al, we calculated mean measurement errors as the standard deviations of landmark coordinates, which we considered to be sufficiently low as long as the errors were smaller than the voxel size (<0.38 mm) along the x, y, and z dimensions.
Geometric morphometrics describes a mathematical approach to the quantification, statistical multivariate analysis, and visualization of 3D shape variations, including the modeling of the effects of the covariates (age, size, and so on). For the Procrustes superimposition, raw coordinate (x, y, z) configurations were aligned to the group centroid, scaled to a common centroid size of one, and rotated to minimize squared deviation in the software MorphoJ (version 1.05f). Because the purpose of these analyses was to test covariation under the null hypothesis of independence, external and internal data sets were treated as individual blocks in different shape spaces. For asymmetry, the Procrustes superimposition was modified to estimate the asymmetric component of shape, which is the deviation from the expectation of perfect right-left symmetry of paired landmarks across midline landmarks.
Statistical analysis
Partial least squares (PLS) was used to assess whether shape variation significantly covaries between external and internal datasets. We analyzed both Procrustes and asymmetric component data with PLS. PLS examines patterns of covariation between 2 or more sets of variables. We performed a 2-block PLS analysis, a widely used method in geometric morphometrics that is based on the singular value decomposition of the matrix of covariances between 2 sets of variables: face and skeleton. Pairs of new axes are derived as linear combinations of the original variables. As with ordination methods, PLS axes are uncorrelated, with the first pair accounting for the greatest amount of interblock covariation, the second pair for the next greatest amount, and so on. The amount of covariation between the 2 blocks of variables is measured by the R v coefficient, which is a multivariate analog of the squared correlation. Statistical significance was tested via permutation (10,000 replicates) under the null hypothesis of complete independence between the 2 blocks of variables.
To assess the correspondence of changes in shape associated with age-related and size-related changes for each data set, we performed an independent multivariate regression on both centroid size (the average of the summed distances of each landmark from the configuration centroid) and age measured in years. Multivariate regression is a technique for predicting the values of at least 1 dependent variable from the values of at least 1 independent variable. To compare the similarity of growth between the data sets, we modeled internal shape scores as a function of external shape scores using a generalized linear model and tested these against the null hypothesis of no correlation. Since both measures were estimated with error, we performed regressions using reduced major axes and evaluated 95% confidence intervals in the smatr3 package implemented in R 3.0.2.
Results
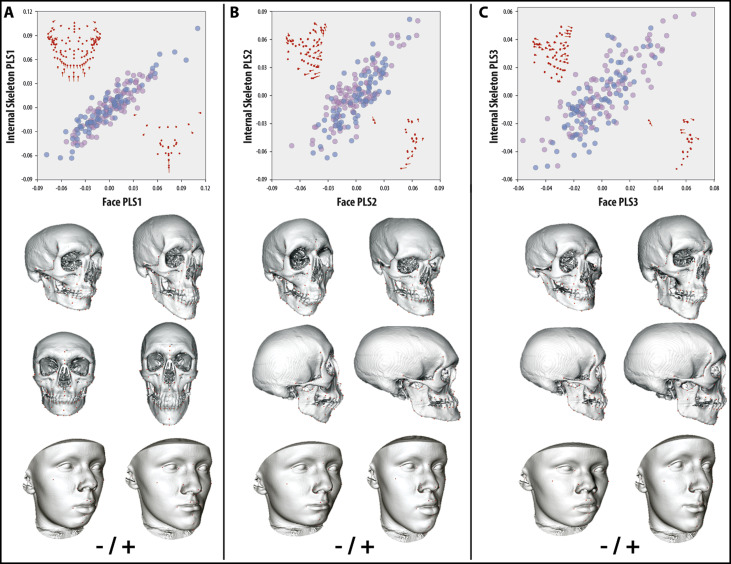
For the shape analysis, mean measurement errors caused by thresholding or landmarking were low relative to voxel size (x = 0.33 mm; y = 0.29 mm; z = 0.34 mm). Analysis of internal and external shape covariation indicated a highly significant relationship overall ( R v = 0.560; P <0.0001), comparable with previous 2-dimensional studies and independent of sex. Individual PLS axes showed similarly high correlations ( Supplementary Table S2 ). PLS 1-13 accounted for 98.7% of total covariation between data sets, and all had singular values with high significance ( P <0.0001) and correlations that ranged from 0.92 to 0.64 ( P <0.0001). Based on a scree analysis, it is likely that axes beyond PLS 6 (>2% total covariation) are indistinguishable from background or error variation at this sample size. Examination of PLS 1-3 demonstrated coordinated shape changes between internal and external data sets (ie, regional landmark displacements had similar direction and magnitude), supporting the hypothesis that surface morphology accurately predicts skeletal shape ( Fig 1 , A-C).