Dental care in the operating room requires expertise to be efficient, effective, and comprehensive. By gathering appropriate information preoperatively, intraoperatively, and postoperatively, the dentist can assume the leadership role that is required for effective dental care. Standardizing procedures, while including the training of residents, can meet the dental goals for comprehensive dental management.
Provision of dental care under general anesthesia for special needs patients requires evaluation of the patient both from a dental and a medical perspective. The dental patient must be screened for the necessity of dental care since there are inherent risks associated with the administration of general anesthesia. The goals of the medical assessment include comprehensive review of the past medical history, previous surgical history, and review of current and past medications. The dental assessment requires obtaining enough information concerning dental pathology to justify the provision of dental care under general anesthesia if the patient is not cooperative for care under local anesthesia in the outpatient setting.
The registration process can be time-consuming and disruptive for an uncooperative patient. In an established practice that facilitates the provision of care for the special needs patient it is more efficient to obtain copies of the demographic and insurance information, medical history, and necessary general consents before the initial dental screening visit. Information about the guardianship status is also needed. Forms may be mailed to the families/caregivers following the initial contact. Once the registration paperwork is completed and returned, the appointment can be scheduled. Of course, when there is an emergent situation every attempt must be made to expedite this process.
Medical history
It is essential to obtain an accurate medical history. An evaluation for pre-existing medical conditions must be performed before any therapeutic measures. Because patients may be living apart from family, obtaining the history may require collating information from multiple sources. Patients who live at home with parents/family often have had ongoing medical care from physicians with whom the family has developed a close relationship. In that case, obtaining accurate information is easier because there is continuity. When patients are living in group homes or with a sponsor, the individual who is transporting the patient to the dental office often has little or no information concerning the patient. Acquiring information from primary sources is critical to ensure accuracy. Patients residing in group home settings often have a large medical journal that is brought to each dental visit. Copies of the annual physical, current medications, and recent consultations provided in this journal are an excellent resource for the dentist to obtain an accurate medical history, medication reconciliation, and list of current medical providers.
Criteria for dental care under general anesthesia
Patients with special needs require the same level of assessment as regular patients. The assessment includes a comprehensive dental examination of hard and soft tissues, complete radiographs, periodontal charting, and assessment of function and occlusion. If there is limited cooperation from the patient while reviewing the medical history and initiating the assessment, it is important to obtain as much information as possible even if treatment cannot be completed under local anesthesia in the outpatient setting. Sometimes a panoramic film can be taken that provides some insight into treatment requirements. In addition, especially for patients who are in their 20s and 30s, the presence of impacted teeth may necessitate the presence of an oral surgeon for the completion of care under anesthesia.
If patients have not received treatment for a considerable period of time there may be an overwhelming amount of dental care that needs to be provided while the patient is under general anesthesia. Often the oral hygiene is limited or non-existent and the periodontal treatment needs are extensive. Specific documentation about presence of caries, nonrestorable teeth, impactions, significant calculus assists in planning the time for the scheduled care under general anesthesia.
Criteria for dental care under general anesthesia
Patients with special needs require the same level of assessment as regular patients. The assessment includes a comprehensive dental examination of hard and soft tissues, complete radiographs, periodontal charting, and assessment of function and occlusion. If there is limited cooperation from the patient while reviewing the medical history and initiating the assessment, it is important to obtain as much information as possible even if treatment cannot be completed under local anesthesia in the outpatient setting. Sometimes a panoramic film can be taken that provides some insight into treatment requirements. In addition, especially for patients who are in their 20s and 30s, the presence of impacted teeth may necessitate the presence of an oral surgeon for the completion of care under anesthesia.
If patients have not received treatment for a considerable period of time there may be an overwhelming amount of dental care that needs to be provided while the patient is under general anesthesia. Often the oral hygiene is limited or non-existent and the periodontal treatment needs are extensive. Specific documentation about presence of caries, nonrestorable teeth, impactions, significant calculus assists in planning the time for the scheduled care under general anesthesia.
Preoperative flow sheet
Once it is determined that care under anesthesia is required, an organized approach to scheduling reduces the time required for the support staff, and is essential for procedures taking place in the operating room (OR).
The flow sheet should include
- 1.
Patient name, date of birth, and medical record number
- 2.
Current address and phone number of home or facility where patient resides
- 3.
Contact person and phone/cell phone number
- 4.
Guardian name, address, and phone number
- 5.
Insurance company, address, phone number, plus copy of insurance card
- 6.
Date and time scheduled for the OR
- 7.
Confirmation number from the OR
- 8.
Name of dentist
- 9.
Name, address, and phone number of primary care physician
- 10.
Place for additional notes concerning the case
Providing all of the above information on one form assists every individual who is involved in the case. If the person who does the scheduling is not available, having this information accessible for another staff person to review is invaluable.
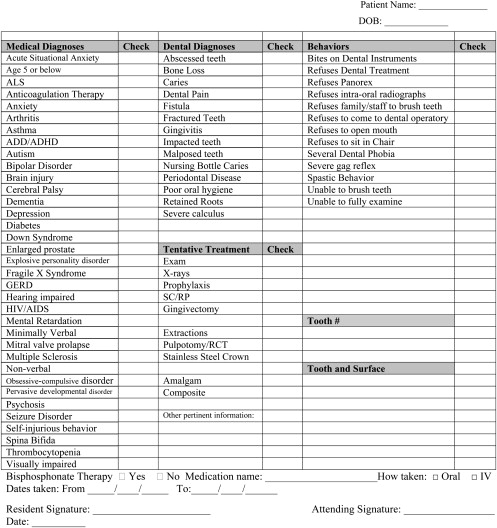
Since the advent of precertification by insurance companies, preformatted forms for additional information can reduce the need to write individual letters and descriptions. The second part of the preoperative evaluation includes a checklist of medical diagnoses/conditions, dental diagnoses, behaviors in the dental setting, and a tentative treatment plan. When signed by the providing dentist. this document can be used for precertification for facility charges as well as the dental charges. Figs. 1 and 2 provide examples of a preoperative flow sheet and a preoperative medical/dental checklist.
Patient scheduling
Each institution that provides dental care under general anesthesia has rules and regulations concerning appropriate timing of hospital, surgical, and anesthesia consent, medical clearance, and laboratory testing.
Consent
The risks, benefits and alternatives to treatment—including no treatment—must be included as part of the discussion for the consent.
It is imperative to determine who gives consent for the procedures. If guardianship has been established, a copy of the guardianship papers should be obtained. Higher functioning patients may be able to sign their own consents. Because many patients are accompanied by staff if they are residing in a group home setting, it is appropriate to ask if the patient has any relatives whom they want to inform about the scheduled procedures. With HIPAA regulations it is mandatory to get the patient/guardian’s consent before discussing the details of care with other individuals. In addition, the consent is only valid for a finite period of time, which is stipulated by the rules and regulations of the hospital/surgical center where the procedure is taking place.
Among older patients and their elderly parents it is sometimes difficult to obtain consent. The discussion about who gives consent and how readily it can be obtained needs to occur during the presurgical screening. If a face-to-face discussion and signing of the consent is not possible, attempts should be made to call the guardian to discuss the proposed procedure. If that fails, then a cover letter describing the procedure in detail with information on how to contact the treating dentist for questions should be sent to the guardian along with the consent forms. The group home staff often has detailed information on the availability of the guardians and whether the consent should be mailed directly to the guardian or given to the group home staff for signature when the guardian visits the patient. Again, a written description of proposed procedures is required.
Medical Clearance
A preoperative history and physical must be obtained within a defined period of time before the surgical procedure. Again, the hospital/surgical center will stipulate that time frame in their rules and regulations. If the hospital has guidelines for presurgical testing, this should be included in the packet of materials that are given to the patient and any guardians/staff who accompany the patient to the medical visit.
Anesthesia Consent
Depending on the facility there may be a separate anesthesia consent that must be signed before the initiation of the dental case.
Facility Scheduling
Arrangements must be made with the facility where the dental case is to be completed.
Information for elective dental cases require
- 1.
The requested date and time of the operation
- 2.
Condition of patient
- 3.
Type of operative procedure
- 4.
Length of operation
- 5.
Type of anesthesia
- 6.
Type of admission (eg, inpatient, outpatient, day surgery)
- 7.
Special equipment
Once this information is obtained a specific time/date is scheduled.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


