Introduction
The purpose of this article was to test the theory that short miniscrews will decrease the possibility of damaging the root, but the failure rate will increase.
Methods
One hundred eighty-six miniscrews (diameter, 1.3 × 5 mm, n = 63; 6 mm, n = 62; 7 mm, n = 61) were placed in 105 consecutive patients. Multislice computed tomography and cone-beam computed tomography scans were taken before and after miniscrew placement. Insertion torque was measured at miniscrew placement.
Results
The success rate of the miniscrews in the maxilla (93.4%) was higher than that in the mandible (70.3%). A significantly lower success rate with 5-mm miniscrews was observed compared with 6-mm and 7-mm miniscrews in the mandible. Miniscrews placed in less than approximately 3.8 mm of bone and those within 1.4 mm of the root had significantly higher failure rates. Miniscrews placed with insertion torque greater than 10 Ncm had a tendency for a lower success rate.
Conclusions
The optimum lengths of miniscrews of a diameter of 1.3 mm are 5 mm in the maxilla and 6 mm in the mandible. They should be placed at a distance from the root with insertion torque less than 10 Ncm for safe orthodontic anchorage without failure.
Recently, miniscrews have been routinely used as orthodontic anchorage, since absolute anchorage is possible without patient cooperation. Miniscrews are widely accepted by orthodontists because of their small size and minimum surgical intervention. Furthermore, short miniscrews can be placed in various regions in the alveolar bone, resulting in effective control of tooth movement in both anteroposterior and vertical directions; however, since miniscrews are placed between roots, damage to the neighboring root has been the greatest problem with their use. In particular, long miniscrews are associated with greater incidences of sinus bicortical perforations. In addition, miniscrews are also used as anchorage in palatal areas, where they have greater stability because of the dense cortical bone that can prevent root contact.
Several studies have focused on preventing root damage with miniscrews. Several studies have evaluated safe zones for placing miniscrews without root damage and also in the palate. The use of a surgical stent is also recommended to prevent root damage ; however, reducing the length might be the most effective and practical way to prevent root damage.
Reducing the length of the miniscrew would markedly decrease the possibility of damaging or touching the neighboring roots; however, the failure rate might increase with decreased mechanical strength by using short miniscrews. Several investigations related to miniscrew failure have been previously reported. One suggested factor for miniscrew failure is the diameter of the miniscrew. Two studies that compared the failure rates between miniscrews of 2 diameters of the same type and length concluded that a smaller diameter resulted in greater stability. With a larger diameter, the proximity of the miniscrew to the root increases and might result in failure of the miniscrew. On the other hand, the length of the miniscrew has been suggested to have less effect on the failure rate. However, if root proximity is a factor for failure, reducing the length of the miniscrew might decrease its proximity to the root and reduce the failure rate. It is not clear whether there is a direct relationship between the length of the miniscrew and these suggested failure factors.
Cone-beam computed tomography (CBCT) has been used for treatments involving miniscrews in orthodontics. To assess the ideal location for miniscrew placement, measurements of spaces between roots and cortical bone thickness have been analyzed. Another suggested factor failure for miniscrews is bone density ; however, Hounsfield units (HU) in CBCT are known to have low repeatability and lower reliability for the measurement of bone density than multislice computed tomography (MSCT). Thus, we also used MSCT to measure bone density in this study.
In this study, to estimate the shortest miniscrew for safe use as orthodontic anchorage with sufficient ability to resist orthodontic forces, failure factors such as cortical bone thickness (including the total length of the miniscrew in the bone), bone density, root proximity, and placement torque were analyzed for 3 lengths (5, 6, and 7 mm) of miniscrews by CBCT and MSCT.
Material and methods
One hundred five consecutive patients (30 male, 75 female; mean age, 20.9 years; range, 13.1-32.4 years) in whom 186 miniscrews (122 in the maxilla, 64 in the mandible) were placed for anchorage in Tohoku University Hospital in Sendai, Japan, from March 2009 to May 2010, fulfilling the inclusion criteria, were used for analysis. The inclusion criteria were patients in the permanent dentition with a minimum age of 13 years at the beginning of treatment and whose planned treatment included at least 2 miniscrews placed between the second premolar and the first molar for maximum anchorage. Exclusion criteria were previous orthodontic treatment, craniofacial anomalies, and surgical patients.
All patients consented to participate in this study. An unstratified subject allocation sequence was generated by a computer program; the patients were randomly assigned to 3 groups (patients with 5-mm and 6-mm miniscrews in either side of the jaw, patients with 5-mm and 7-mm miniscrews, and patients with 6-mm and 7-mm miniscrews); the groups were well balanced for sex, age, and Angle classification ( Table I ). The study protocol was reviewed and approved by the institutional board of Tohoku University.
| Maxilla (n = 122) | Mandible (n = 64) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5- and 6-mm screws | 6- and 7-mm screws | 5- and 7-mm screws | 5- and 6-mm screws | 6- and 7-mm screws | 5- and 7-mm screws | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Age (y) | 21.4 | 4.9 | 21.2 | 5.7 | 20.6 | 5.2 | 22.5 | 5.3 | 21.8 | 6.7 | 21.6 | 5.7 |
| Male (%) | 29.4 | – | 27.8 | – | 29.4 | – | 27.8 | – | 29.4 | – | 27.8 | – |
| Female (%) | 70.6 | – | 72.2 | – | 70.6 | – | 72.2 | – | 70.6 | – | 72.2 | – |
| Angle class (%) | ||||||||||||
| I | 39.0 | – | 42.0 | – | 40.0 | – | 40.0 | – | 41.0 | – | 39.0 | – |
| II | 45.0 | – | 46.0 | – | 45.0 | – | 49.0 | – | 44.0 | – | 45.0 | – |
| III | 16.0 | – | 12.0 | – | 15.0 | – | 11.0 | – | 15.0 | – | 16.0 | – |
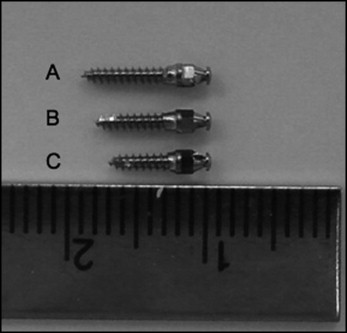
The miniscrews (AbsoAnchor; Dentos, Daegu, Korea; diameter, 1.3 mm: length, 5 mm, n = 63; 6 mm, n = 62; 7 mm, n = 61) were installed under local anesthesia between the second premolar and the first molar by 2 orthodontists (second and fourth authors) ( Fig 1 ). The screw hole was made with a 1.0-mm round bur and a drill (diameter 1.1 × 5.0 mm) at 500 rpm, and the miniscrew was placed with the self-tapping method. Insertion torque was measured and recorded at placement with an AbsoAnchor torque screwdriver. All miniscrews were immediately loaded with 50 to 100 g of orthodontic force with a nickel-titanium closed-coil spring (Sentalloy; Tomy, Tokyo, Japan). Miniscrews that were mobile or failed within 6 months of placement were defined as failures.
MSCT scans were made with a Somatom Definition (Siemens, Forchheim, Germany) with an 0.8-mm slice increment, a 1.0-mm slice thickness, and a 512 × 512 mm matrix for preminiscrew implantation. A stent made from paraffin and a gutta-percha point was used during the preimplantation MSCT. CBCT (3D-Accuitomo; J. Morita, Kyoto, Japan) was performed (80-90 mVp; 3.5-5 mA; scanning time, 17.5 seconds; field of view, 60 × 60 mm; voxel size, 0.125 mm) after miniscrew implantation.
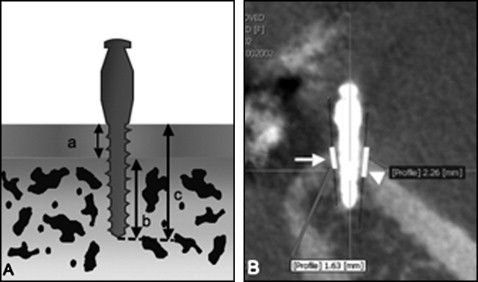
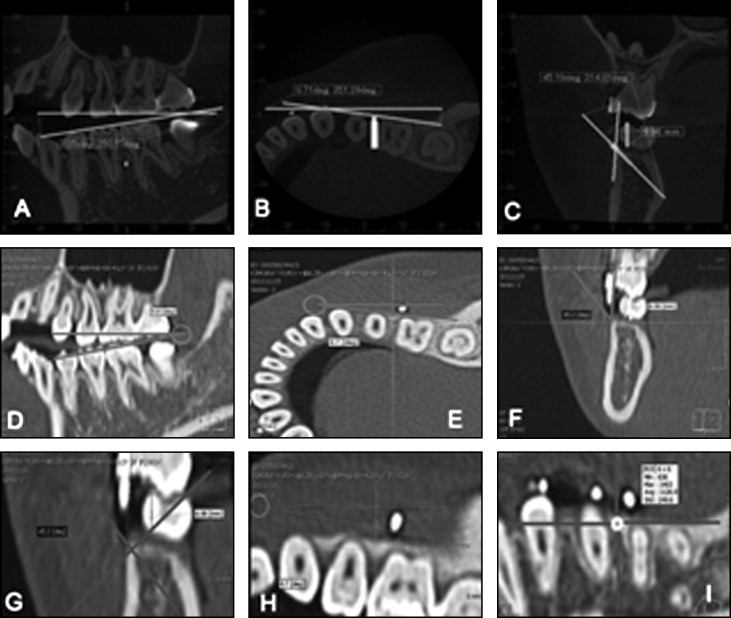
For the cortical bone thickness (total bone) and the bone density measurements, the CBCT or computed tomography data were converted into DICOM files and analyzed using OnDemand3D software (CyberMed, Seoul, Korea). Cortical bone thickness and total bone length ( Fig 2 ) were measured in the sagittal and coronal planes, which ran parallel to the long axis of the miniscrew at 2 points (upper and lower) on the 3-dimensional images. For the bone density measurements, the angle between the cortical bone and the miniscrew was measured on a postimplantation multiplanar reformatted image ( Fig 3 , A-C ). The angle and the location of the miniscrew were projected onto a preimplantation MSCT image ( Fig 3 , D-F ) to identify the insertion point of the miniscrew. Hounsfield units were measured by reconstructing the horizontal plane perpendicular to the long axis of the miniscrew in the center of the cortical bone (region of interest, 14 × 14 HU) ( Fig 3 , G-I ).
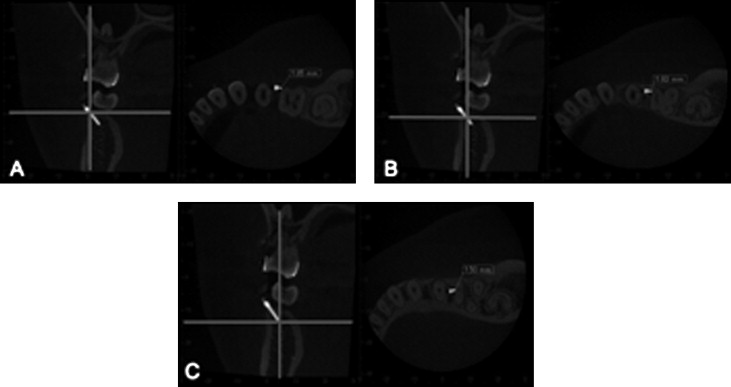
Measurements of root proximity and the miniscrew were analyzed using One Data Viewer software (J. Morita) and multiplanar reformatted postimplantation CBCT images. The multiplanar reformatted images were made by slicing in the coronal direction, passing through the long axis of the miniscrew (slice interval, 0.25 mm; slice thickness, 0.5 mm). The measurement was made from the nearest root to the miniscrew. Furthermore, we determined 3 points (head of the miniscrew, Fig 4 , A ; midpoint, Fig 4 , B ; and apex, Fig 4 , C ) and measured the distance from these points to the root surface in the horizontal plane. The average length of these 3 points was analyzed.
Statistical analysis
Statistical analysis was performed using the Mann-Whitney U test to examine differences among root proximity, cortical bone thickness, bone density, and insertion torque value. P <0.05 was considered significant. These analyses were carried out with statistical analysis software (Statview; SPSS, Chicago, Ill). In addition, the receiver operating characteristics curve was computed by JMP 10 (SAS Institute Japan, Tokyo, Japan) to determine the optimal cutoff values of total bone length and root proximity to distinguish failed and successful miniscrews.
Results
The success rates were 93.4% and 70.3% in the maxilla and the mandible, respectively ( Table II ). In the maxilla, there were no significant differences in the success rates between the length or the right and left sides. On the other hand, in the mandible, a significantly lower success rate with the 5-mm screws was observed compared with the 6-mm and 7-mm screws. No significant difference was observed between the right and left sides. In addition, no miniscrew penetrated the root or the sinus by CBCT evaluation; therefore, all miniscrew sizes (diameter, 1.3 mm; length, 5-7 mm) used in this study can be safely used between the second premolar and the first molar.
| Maxilla | Mandible | |||||
|---|---|---|---|---|---|---|
| Total (n) | Fail (n) | Success (%) | Total (n) | Fail (n) | Success (%) | |
| 5 mm | 41 | 2 | 95.0 | 22 | 11 | 50.0 ∗ |
| 6 mm | 41 | 4 | 90.2 | 21 | 5 | 76.2 |
| 7 mm | 40 | 2 | 95.0 | 21 | 3 | 85.7 |
| Right | 61 | 5 | 91.8 | 32 | 11 | 65.6 |
| Left | 61 | 3 | 95.1 | 32 | 8 | 75.0 |
| Total | 122 | 8 | 93.4 | 64 | 19 | 70.3 |
The total average cortical bone thicknesses were 1.6 and 1.9 mm in the maxilla and the mandible, respectively ( Table III ). There were no significant differences in the success rates between the lengths or the right and left sides in both jaws.
| Maxilla (mm) | Mandible (mm) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cortical | Trabecular | Total bone (mm) | Cortical | Trabecular | Total bone (mm) | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Success | 1.6 | 0.3 | 3.1 | 0.5 | 4.7 | 0.7 | 1.9 | 0.4 | 2.6 | 0.5 | 4.5 | 0.8 |
| Fail | 1.6 | 0.3 | 2.7 | 0.3 | 4.3 | 0.3 | 2.0 | 0.5 | 2.0 ∗ | 0.5 | 4.0 ∗ | 0.7 |
| 5 mm | 1.6 | 0.3 | 2.5 | 0.5 | 4.1 | 0.5 | 1.8 | 0.4 | 1.8 † | 0.4 | 3.6 † | 0.4 |
| 6 mm | 1.6 | 0.3 | 3.1 | 0.5 | 4.7 | 0.5 | 2.0 | 0.4 | 2.5 | 0.4 | 4.5 | 0.5 |
| 7 mm | 1.7 | 0.3 | 4.1 | 0.3 | 5.8 | 0.3 | 1.9 | 0.4 | 3.9 | 0.3 | 5.8 | 0.3 |
| Right | 1.5 | 0.3 | 3.0 | 0.7 | 4.5 | 0.7 | 1.8 | 0.4 | 2.4 | 0.5 | 4.2 | 0.7 |
| Left | 1.7 | 0.3 | 3.1 | 0.7 | 4.8 | 0.7 | 1.9 | 0.4 | 2.7 | 0.7 | 4.6 | 0.9 |
∗ Significant difference compared with success group ( P <0.05).
† Significant difference compared with screws of 6 and 7 mm ( P <0.05).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


