Introduction
Our objectives were to evaluate marginal alveolar bone height in the anterior mandible after orthodontic treatment and to assess any correlations between morphologic and treatment changes.
Methods
We used 57 pretreatment and posttreatment cone-beam computed tomography images (17 male and 40 female subjects; 22 Class I, 35 Class II; average age, 18.7 ± 10.8 years; average treatment time, 22.7 ± 7.3 months) to measure cortical bone thickness, ridge thickness, distance from the apex to the labial cortical bone, and the distance from the cementoenamel junction to the marginal bone crest. Changes in the cementoenamel junction to the marginal bone crest distance were correlated with pretreatment measurements and treatment changes.
Results
Although there were great variations, the average facial and lingual vertical bone losses were 1.16 ± 2.26 and 1.33 ± 2.50 mm, respectively. The incisor-mandibular plane angle changes were also highly variable, averaging 2.4°.
Conclusions
Orthodontic treatment causes changes in alveolar bone height and cortical bone thickness around the mandibular incisors. Although pretreatment cortical bone thickness, ridge width thickness, and specific tooth movements all play roles in what happens to the bone during treatment, incisor inclination was not correlated with alveolar bone height changes.
Highlights
- •
Orthodontic treatment causes changes in alveolar bone height around the mandibular incisors.
- •
It also causes changes in cortical bone thickness around the mandibular incisors.
- •
Cortical bone and ridge width thickness affect bone during treatment.
- •
Incisor inclination was not correlated with alveolar bone height changes.
The tissue response to orthodontic forces can lead to gingival inflammation, alveolar bone loss, damage to the tooth enamel surfaces, pulpal reactions, root resorption, and marginal bone loss. Many studies have evaluated the effects of orthodontic treatment on alveolar bone height.
Most studies evaluating alveolar bone height have used bitewing or periapical radiography and have focused on the posterior dentition. The advent of cone-beam computed tomography (CBCT) has allowed for more extensive studies evaluating alveolar bone height in the anterior region. Sarikaya et al, who evaluated patients requiring retraction of the maxillary incisors to close extraction spaces, found that the lingual alveolar bone thickness decreased significantly; in 11 of 19 patients, at least 1 incisor was outside the alveolar bone at the crest level. Lund et al, who also evaluated premolar extraction patients, found that 84% of the lingual surfaces of the mandibular central incisors demonstrated bone height decreases of more than 2 mm, with average decreases of 5.7 mm on the lingual aspect and increases of 0.8 mm on the buccal aspect of the same tooth.
Experimental evidence suggests that vertical bone loss can also occur when mandibular incisors are proclined. Steiner et al found that in monkeys, moving the mandibular incisors labially by 3.05 mm caused 5.48 mm of marginal bone loss. Also using monkeys, Batenhorst et al reported 7 mm of bone loss associated with 6 mm of incisor proclination. Similar studies with human subjects have yet to be performed.
Because of the lack of human studies, the purpose of this study was to evaluate how changes of incisor position affect marginal alveolar bone height using CBCT. A secondary purpose was to evaluate any associations between initial bone characteristics and changes in bone characteristics with the amount of vertical alveolar bone height changes.
Material and methods
The study was based on pretreatment and posttreatment CBCT images of 57 patients who had nonextraction treatment by 1 practitioner. The CBCT images were taken with an i-CAT CBCT machine (Imagining Sciences International, Hatfield, Pa). The scans were taken in a single 360° rotation at a scan time of 4.8 seconds, 120 kVp, 0.3-mm voxel size, and 536 × 536 mm field of view.
A total of 114 CBCT images (57 pretreatment, 57 posttreatment) pertaining to 17 male and 40 female subjects, ages 18.7 ± 10.8 years, were used. Of the 57 subjects, 22 had Class I and 35 had Class II malocclusions. Patients were excluded if they had (1) missing or unerupted mandibular permanent incisors, (2) periapical or periradicular pathologies or radiolucencies of either periodontal or endodontic origin, (3) a significant medical or dental history (eg, use of bisphosphonates or bone altering medications, or diseases), and (4) poor image quality.
All patients were treated with self-ligating Damon Q brackets (Ormco, Orange, Calif) with a 0.022-in slot. Initial leveling and aligning were performed using round (0.014 and 0.018 in) and rectangular (0.014 × 0.025 in, and 0.018 × 0.025 in) heat-activated nickel-titanium archwires. Finishing archwires consisted of rectangular (0.019 × 0.025 in) stainless steel wires. The mean treatment duration was 22.7 ± 7.3 months.
Each CBCT scan was imported into the software (version 11.0; Dolphin Imagining & Management Solutions, Chatsworth, Calif) for analysis. With the 3-dimensional image oriented along the Frankfort horizontal plane, lateral cephalograms were constructed with the midline bisecting the mandibular right central incisor, thus creating an image representing the left half of the craniofacial complex.
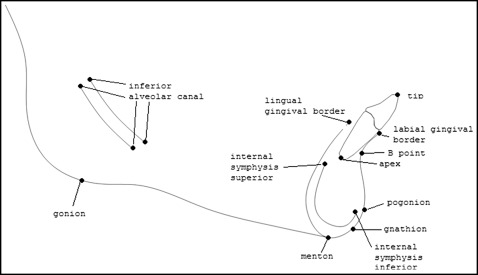
From the constructed lateral cephalograms, the following structures and landmarks were identified and traced: mandibular right incisor tip, mandibular right incisor apex, labial gingival border, lingual gingival border, inferior alveolar canal (4 points), internal border of the symphysis (superior and inferior), B-point, pogonion, gonion, gnathion, and menton ( Fig 1 ). The incisor-mandibular plane angle (IMPA), the angle formed by the intersection of the long axis of the mandibular incisor and the gonion-menton line, was measured. The pretreatment and posttreatment mandibles were then superimposed using stable structures as described by Bjork and Skieller. From the superimpositions, the x and y coordinates of each point were obtained, with pogonion as the origin and orienting along the Frankfort horizontal plane. The coordinates were used to calculate the angular differences between the pretreatment and posttreatment incisor positions. The coordinate system was also used to calculate the anteroposterior distances that the apex and the incisor tip moved.
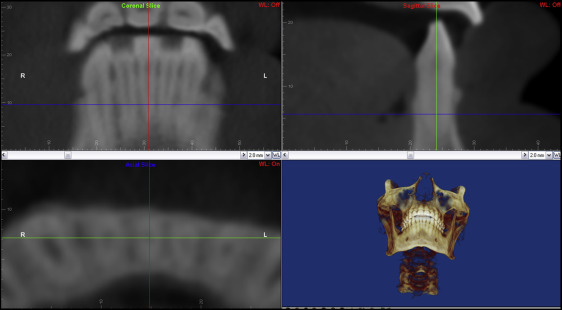
To examine the morphologic features of the alveolar bone, each CBCT image was oriented along the long axis of the mandibular right central incisor (bisecting the pulp and the canal) in the sagittal and coronal planes, and bisecting the canal in a labiolingual direction in the axial plane at the same time ( Fig 2 ). Only the right side was measured because there are no side differences in cortical bone thickness. Once oriented, a sagittal cross section of the mandibular right incisor was produced. From this image, measurements from the labial (F-CEJ-MBC) and lingual (L-CEJ-MBC) aspects were made from the most apical portion of the cementoenamel junction (CEJ) to the most coronal aspect of the marginal bone crest ( Fig 3 , A ).
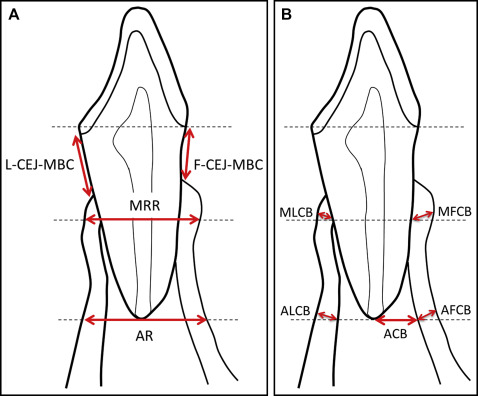
From the height of the labial CEJ point, a horizontal line was made. From this line, a vertical distance from the labiolingual midpoint of the pulp canal to the apex of the root was measured. This distance was halved, and a horizontal was drawn demarking the height at which the midroot-level ridge thickness (MRR) ( Fig 3 , A ) and midroot-level cortical bone thickness (MLCB and MFCB) were measured ( Fig 3 , B ). Another horizontal line was drawn at the height of the apex. This height was used to measure apex-level ridge thickness (AR) ( Fig 3 , A ), cortical bone thickness (ALCB and AFCB), and distance (ACB) from the apex to the internal border of the labial cortical bone ( Fig 3 , B ).
Cortical bone thickness was measured as the line from the point where the horizontal line intersected the internal border of the cortical plate, perpendicular to the external border of the cortical plate.
Technical reliability of the measurements was based on 2 replicate measurements of 40 pretreatment or posttreatment records, which were randomly selected from the larger sample. Random error was quantified using the method-error statistic, calculated with the following formula:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


