Introduction
The aim of this 2-arm parallel trial was to evaluate enamel demineralization after rapid maxillary expansion (RME) compared with an untreated control group using quantitative light-induced fluorescence.
Methods
Thirty-six patients who needed RME as part of their orthodontic treatment were separated randomly into either the control group or the intervention group (RME). Eligibility criteria included crossbite, no previous orthodontic treatment, no systemic disease, and all permanent teeth erupted except second and third molars. The main outcome was quantitative evaluation of demineralization, and assessment of the vulnerability of each tooth to demineralization was the secondary outcome. Randomization was made at the start of the study with preprepared random number tables. Blinding was applicable for outcome assessment only. Patients in the RME group underwent expansion with a bonded acrylic expander; patients in the control group were untreated. Records were taken using quantitative light-induced fluorescence Digital Biluminator (Inspektor Research Systems, Amsterdam, The Netherlands) in pretreatment and posttreatment observation phases. The presence and extent of lesions on the buccal surfaces of all teeth, except the second and third molars, were assessed. The fluorescence loss, lesion area, and percentage of fluorescence loss were determined using the system’s software. The numbers of teeth with more than a 5% change in fluorescence loss, were calculated. Data were analyzed with Wilcoxon signed rank, Mann-Whitney U, multivariate analysis of variance, and chi-square tests ( P <0.05). Risk and odds ratios were calculated.
Results
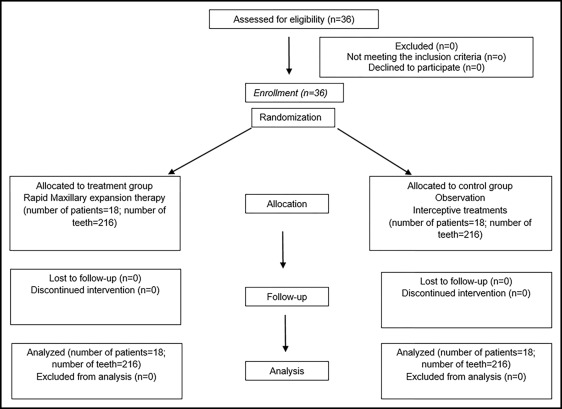
A total of 36 patients were randomized to either the RME or the control group in a 1:1 ratio. This study was completed with 18 patients in the RME group (8 girls, 10 boys; mean age, 14.2 ± 1.0 years) and 18 patients in the control group (10 girls, 8 boys; mean age: 14.1 ± 0.8 years). All patients completed the study, and none were lost to follow-up. The area of demineralization decreased in the RME group (−17.50 mm 2 ), which was a significantly greater decrease than in the control group (0.00) (effect size, −2.63; mean difference, −87.94; 95% confidence interval, −223.75-47.86; P = 0.008). No statistically significant difference was found for fluorescence loss. The numbers of teeth with demineralization and remineralization were higher in the treatment group. According to the risk ratio, the difference between groups regarding demineralization was not significant. No harm was found except gingivitis associated with the bonded appliance.
Conclusions
RME therapy using a bonded expander does not increase enamel demineralization.
Registration
This trial was not registered.
Protocol
The protocol was not published before trial commencement.
Highlights
- •
Decalcification after rapid maxillary expansion (RME) was examined with quantitative light-induced fluorescence.
- •
Areas of demineralization decreased after RME with a bonded appliance.
- •
There was no statistically significant difference in fluorescence loss in treatment vs control groups.
- •
The numbers of teeth with demineralization and remineralization increased in treatment group.
- •
There were no significant differences in frequency of demineralization for each tooth.
Rapid maxillary expansion (RME) is used to correct posterior crossbites, improve smile esthetics, and increase arch length and airway clearance. With RME, the midpalatal suture is separated, cell activity increases in the suture area, and bone is gained in the transversal plane.
The appliances used for RME are 2 types: bonded and banded. Bonded RME appliances have been often preferred recently because the rigidity of the bonded RME appliance causes less tipping of the teeth. The appliance consists of a screw in the middle of the palate and an acrylic cap that covers the teeth. Because the sutural organization has been affected by RME, reorganization necessitates a long retention period.
Wearing the appliance during the active treatment period and the retention phase makes it more difficult for patients to establish proper oral hygiene; this causes microbial plaque accumulation. For this reason, expansion seems to increase the demineralization risk. Demineralization results in compromised esthetics and may require invasive intervention, with additional financial, emotional, and biologic costs to patients and their families, and a frustrating clinical dilemma for orthodontists.
Quantitative light-induced fluorescence (QLF) is a new technique for the detection of early mineral changes in enamel. The fluorescence image of enamel with early lesions can be digitized, and the fluorescence loss in the lesion can then be quantified in relation to the fluorescence radiance level of sound enamel. Recent studies indicate that QLF is suitable for in-vivo monitoring of mineral changes in early enamel lesions. Furthermore, the use of QLF as a method of following caries development during orthodontic treatment has been suggested for quantitative judgment of the same lesion at different times.
Although there have been many studies in the orthodontic literature to evaluate enamel demineralization around orthodontic brackets, to our knowledge no study in the literature has evaluated the demineralization effect of RME using a bonded acrylic appliance. Because of the limited research available in this area, the aim of this study was to evaluate enamel demineralization after RME using the QLF method in vivo.
Specific objectives or hypotheses
In this study, we tested the hypotheses that (1) there is no difference between RME-treated and untreated subjects regarding the amount of demineralization quantitatively, (2) the numbers of teeth showing demineralization do not differ between RME-treated and untreated subjects, and (3) there is no difference between teeth regarding their vulnerability to enamel demineralization.
Material and methods
Trial design
This was a 2-arm parallel-group, randomized, controlled trial with a 1:1 allocation ratio.
Participants, eligibility criteria, and settings
Approval of the medical ethical committee of Izmir Katip Celebi University, Izmir, Turkey was obtained for this study (number 64). The participants were selected from those who needed to be treated with RME and put on the waiting list of the orthodontic department’s clinic. The sample comprised 36 patients. The inclusion criteria were as follows: (1) unilateral or bilateral crossbite caused by a transversal maxillary deficiency, (2) no previous orthodontic treatment, (3) no systemic disease, and (4) all permanent teeth erupted except second and third molars.
Interventions
In the first group, RME was applied until the palatal cusps of the maxillary molars and the buccal cusps of the mandibular molars were in the same plane transversally. The patients in the control group were not treated in the first phase, and the observation period was 6 months. During the observation period, interceptive treatments were performed in the control group; immediately after that, their orthodontic treatment was initiated. This study was completed with 18 patients in the treatment group (8 girls, 10 boys; mean age, 14.2 ± 1.0 years) and 18 patients in the control group (10 girls, 8 boys; mean age, 14.1 ± 0.8 years). The flow of the patients through the trial is shown in Figure 1 .
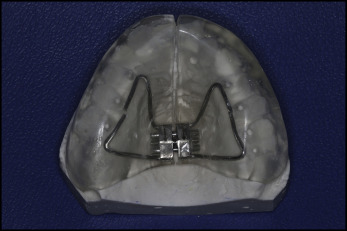
Orthopedic expansion was performed with a bonded type of RME appliance ( Fig 2 ). A hyrax screw (Dentaurum, Pforzheim, Germany) was placed between the second premolars. The palate was covered with acrylic, which extended to the occlusal and middle thirds of the buccal surfaces of the teeth. This appliance was bonded to the maxillary dentition with glass ionomer cement (Ketac Cem Radiopaque; 3M ESPE Dental Products, Neuss, Germany). The screw activation was a quarter turn twice for the first week and a quarter turn per day after that. When the desired amount of expansion was achieved, the screw was stabilized with a ligature wire and kept in the mouth passively for a month. The patients were instructed to wear a Hawley appliance for the rest of their retention period. At 6 months, the QLF recordings were performed in treatment and control groups.
Records were taken using a QLF Digital Biluminator (QLF-D, Inspektor Pro; Inspektor Research Systems, Amsterdam, The Netherlands) in the pretreatment and posttreatment observation phases. The QLF-D is an upgraded version of the first product with a modified filter set (D007; Inspektor Research Systems). The system consisted of a special camera connected to a personal computer in which the QLF-D software was installed. Camera settings were optimized for the environment where the photos were taken, and fixed settings (ISO, 1600; shutter speed, 1/30 second) were then locked in the software. The camera was used with a manual focus at the canines for the front teeth and at the second premolars for the posterior teeth. To ensure standardization, the images were captured with the same camera position and from the same angle. The images were processed with the software using video-repositioning techniques according to the manufacturer’s instructions.
Outcomes (primary and secondary) and any changes after trial commencement
The primary outcome in this investigation was the quantitative evaluation of enamel demineralization using the QLF method. The secondary outcome measures were the assessment of enamel demineralization of individual teeth and the determination of whether any tooth is more vulnerable to demineralization.
The presence and extent of lesions on the buccal surfaces of all teeth, except second and third molars, were assessed by the QLF-D software at the pretreatment observation visit and the posttreatment observation visit. Thus, 12 buccal surfaces per subject were assessed at each time point. The analysis of the images involved the placement of an analysis patch in the stained area, ensuring that the borders of the patch fell on sound enamel. The average fluorescence loss, lesion area, and the percentage of fluorescence loss were determined using the system’s analysis software to determine the lesion extent. The decrease in fluorescence was determined by calculating the percentage difference between the actual and reconstructed fluorescence surfaces.
A threshold value was set at a level of 5% fluorescence loss, which showed a minimum 5% fluorescence loss change between first and second measurements. The lesions captured by the QLF-D clinical system were analyzed quantitatively with the QLF-D software.
No changes to the methods or no outcome changes were occurred after trial commencement.
Sample size calculation
A multivariate analysis of variance with 2 outcome variables and 1 factor with 2 levels indicated at least 80% statistical power based on a medium effect size, Cohen’s d = 0.66, (refer to effect size reported in a similar study: Al-Khateeb S, Forsberg CM, de Josselin de Jong E, Angmar-Mansson B. A longitudinal laser fluorescence study of white spot lesions in orthodontic patients. Am J Orthod Dentofacial Orthop 1998;113:595-602; mean difference, 4.02; SD, 3.59) necessitated a minimum sample size of 18 in each group to detect a significant difference between the groups.
Interim analyses and stopping guidelines
Not applicable.
Randomization (random number generation, allocation concealment, and implementation of the random sequence)
When a patient who fulfilled the inclusion criteria attended the clinic, the patient and parents were informed and invited to participate in the study. If the child and the parents consented, the initial records were taken, and each patient was randomized to receive treatment with a rapid palatal expander or to have treatment delayed for at least 6 months. Randomization was done at the start of the study with random number tables prepared using SPSS software (version 20.0; IBM, Armonk, NY). One researcher (S.N.U.) evaluated the patients, and another author (A.B.) enrolled the patients. The allocation sequence was concealed using numbered and sealed opaque envelopes. Thirty-six patients (mean age, 14.1 ± 0.8 years; range, 11.4-16.5 years) were randomized in a 1:1 ratio to either the treatment or the control group.
Blinding
Blinding of either patient or operator was not possible.
Statistical analysis (primary and secondary outcomes, subgroup analyses)
The data acquired were analyzed statistically to evaluate the possible changes between the treated and control groups. All data were entered into SPSS software for the statistical analysis.
To evaluate the cluster effect, the intracluster correlation coefficients (ICC) were calculated for each dependent variable. The ICC values ranged between 9% and 23%, indicating a clustering effect. Although the mixed model takes care of the cluster effect, nonnormal data causes the parametric model to be unreliable. Thus, patient was chosen for unit of analysis instead of the tooth; the mean value per patient was obtained, and these data were analyzed at the patient level.
The normality test of Shapiro-Wilks and the Levene variance homogeneity test were applied to the data. The data were not normally distributed; thus, nonparametric tests were used. Fluorescence losses and areas of demineralization change were evaluated using Mann-Whitney U and Wilcoxon signed rank tests for intergroup and intragroup comparisons, respectively.
Risk ratios and odds ratios were carried out with statistical methods for new lesion development and lesion remineralization. Confidence intervals (95% CI) were also calculated for relative risks.
To compare the percentages of samples that exceeded the 5% fluorescence loss threshold limit in each group, the chi-square test was used. One-way analysis of variance was used to test the differences of fluorescence loss values of each tooth.
Statistical significance was set at P ≤0.05.
Material and methods
Trial design
This was a 2-arm parallel-group, randomized, controlled trial with a 1:1 allocation ratio.
Participants, eligibility criteria, and settings
Approval of the medical ethical committee of Izmir Katip Celebi University, Izmir, Turkey was obtained for this study (number 64). The participants were selected from those who needed to be treated with RME and put on the waiting list of the orthodontic department’s clinic. The sample comprised 36 patients. The inclusion criteria were as follows: (1) unilateral or bilateral crossbite caused by a transversal maxillary deficiency, (2) no previous orthodontic treatment, (3) no systemic disease, and (4) all permanent teeth erupted except second and third molars.
Interventions
In the first group, RME was applied until the palatal cusps of the maxillary molars and the buccal cusps of the mandibular molars were in the same plane transversally. The patients in the control group were not treated in the first phase, and the observation period was 6 months. During the observation period, interceptive treatments were performed in the control group; immediately after that, their orthodontic treatment was initiated. This study was completed with 18 patients in the treatment group (8 girls, 10 boys; mean age, 14.2 ± 1.0 years) and 18 patients in the control group (10 girls, 8 boys; mean age, 14.1 ± 0.8 years). The flow of the patients through the trial is shown in Figure 1 .
Orthopedic expansion was performed with a bonded type of RME appliance ( Fig 2 ). A hyrax screw (Dentaurum, Pforzheim, Germany) was placed between the second premolars. The palate was covered with acrylic, which extended to the occlusal and middle thirds of the buccal surfaces of the teeth. This appliance was bonded to the maxillary dentition with glass ionomer cement (Ketac Cem Radiopaque; 3M ESPE Dental Products, Neuss, Germany). The screw activation was a quarter turn twice for the first week and a quarter turn per day after that. When the desired amount of expansion was achieved, the screw was stabilized with a ligature wire and kept in the mouth passively for a month. The patients were instructed to wear a Hawley appliance for the rest of their retention period. At 6 months, the QLF recordings were performed in treatment and control groups.
Records were taken using a QLF Digital Biluminator (QLF-D, Inspektor Pro; Inspektor Research Systems, Amsterdam, The Netherlands) in the pretreatment and posttreatment observation phases. The QLF-D is an upgraded version of the first product with a modified filter set (D007; Inspektor Research Systems). The system consisted of a special camera connected to a personal computer in which the QLF-D software was installed. Camera settings were optimized for the environment where the photos were taken, and fixed settings (ISO, 1600; shutter speed, 1/30 second) were then locked in the software. The camera was used with a manual focus at the canines for the front teeth and at the second premolars for the posterior teeth. To ensure standardization, the images were captured with the same camera position and from the same angle. The images were processed with the software using video-repositioning techniques according to the manufacturer’s instructions.
Outcomes (primary and secondary) and any changes after trial commencement
The primary outcome in this investigation was the quantitative evaluation of enamel demineralization using the QLF method. The secondary outcome measures were the assessment of enamel demineralization of individual teeth and the determination of whether any tooth is more vulnerable to demineralization.
The presence and extent of lesions on the buccal surfaces of all teeth, except second and third molars, were assessed by the QLF-D software at the pretreatment observation visit and the posttreatment observation visit. Thus, 12 buccal surfaces per subject were assessed at each time point. The analysis of the images involved the placement of an analysis patch in the stained area, ensuring that the borders of the patch fell on sound enamel. The average fluorescence loss, lesion area, and the percentage of fluorescence loss were determined using the system’s analysis software to determine the lesion extent. The decrease in fluorescence was determined by calculating the percentage difference between the actual and reconstructed fluorescence surfaces.
A threshold value was set at a level of 5% fluorescence loss, which showed a minimum 5% fluorescence loss change between first and second measurements. The lesions captured by the QLF-D clinical system were analyzed quantitatively with the QLF-D software.
No changes to the methods or no outcome changes were occurred after trial commencement.
Sample size calculation
A multivariate analysis of variance with 2 outcome variables and 1 factor with 2 levels indicated at least 80% statistical power based on a medium effect size, Cohen’s d = 0.66, (refer to effect size reported in a similar study: Al-Khateeb S, Forsberg CM, de Josselin de Jong E, Angmar-Mansson B. A longitudinal laser fluorescence study of white spot lesions in orthodontic patients. Am J Orthod Dentofacial Orthop 1998;113:595-602; mean difference, 4.02; SD, 3.59) necessitated a minimum sample size of 18 in each group to detect a significant difference between the groups.
Interim analyses and stopping guidelines
Not applicable.
Randomization (random number generation, allocation concealment, and implementation of the random sequence)
When a patient who fulfilled the inclusion criteria attended the clinic, the patient and parents were informed and invited to participate in the study. If the child and the parents consented, the initial records were taken, and each patient was randomized to receive treatment with a rapid palatal expander or to have treatment delayed for at least 6 months. Randomization was done at the start of the study with random number tables prepared using SPSS software (version 20.0; IBM, Armonk, NY). One researcher (S.N.U.) evaluated the patients, and another author (A.B.) enrolled the patients. The allocation sequence was concealed using numbered and sealed opaque envelopes. Thirty-six patients (mean age, 14.1 ± 0.8 years; range, 11.4-16.5 years) were randomized in a 1:1 ratio to either the treatment or the control group.
Blinding
Blinding of either patient or operator was not possible.
Statistical analysis (primary and secondary outcomes, subgroup analyses)
The data acquired were analyzed statistically to evaluate the possible changes between the treated and control groups. All data were entered into SPSS software for the statistical analysis.
To evaluate the cluster effect, the intracluster correlation coefficients (ICC) were calculated for each dependent variable. The ICC values ranged between 9% and 23%, indicating a clustering effect. Although the mixed model takes care of the cluster effect, nonnormal data causes the parametric model to be unreliable. Thus, patient was chosen for unit of analysis instead of the tooth; the mean value per patient was obtained, and these data were analyzed at the patient level.
The normality test of Shapiro-Wilks and the Levene variance homogeneity test were applied to the data. The data were not normally distributed; thus, nonparametric tests were used. Fluorescence losses and areas of demineralization change were evaluated using Mann-Whitney U and Wilcoxon signed rank tests for intergroup and intragroup comparisons, respectively.
Risk ratios and odds ratios were carried out with statistical methods for new lesion development and lesion remineralization. Confidence intervals (95% CI) were also calculated for relative risks.
To compare the percentages of samples that exceeded the 5% fluorescence loss threshold limit in each group, the chi-square test was used. One-way analysis of variance was used to test the differences of fluorescence loss values of each tooth.
Statistical significance was set at P ≤0.05.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


