Learning Objectives
After reading this chapter, the student should be able to:
- 1.
Recognize the incidence of flare-ups.
- 2.
Describe appropriate diagnostic procedures for endodontic emergencies.
- 3.
Describe the initial patient contact and patient management issues.
- 4.
Describe the role of the staff in discriminating between a true emergency and a nonemergent case.
- 5.
Recognize the categories of flare-ups: pretreatment, intervisit, and postobturation.
- 6.
Describe appropriate nomenclature for diagnostic categories of pulpal and periapical pathologic conditions.
- 7.
Describe the causes of flare-ups and their management.
- 8.
Recognize anatomic factors that may lead to more rapid progression of infection.
- 9.
Recognize the importance of profound anesthesia.
- 10.
Describe the potential role of predisposing factors, including genetics, gender, and anxiety, in exacerbations.
- 11.
Use preoperative, intraoperative, and postoperative pharmaceuticals (e.g., anxiolytics, anesthetics, antiinflammatories, analgesics, and antimicrobials) in emergency cases.
Endodontic emergencies represent an important and complex part of clinical practice. Proper diagnosis and treatment require a knowledge of pulp and periapical pathosis and the ability to use the appropriate diagnostic tests. Diagnostic findings must be synthesized with the patient’s medical and dental history and chief complaint to select the best clinical procedures and therapeutics to address the emergency. The clinician must have an understanding of pain mechanisms, local anesthesia, the appropriate use of therapeutics, and patient management skills. Emergencies may occur prior to the inception of treatment, during treatment, or immediately after the canal or canals have been obturated. Clinical, biologic, and predisposing factors associated with flare-ups are reviewed in this chapter.
The immediate goal of an emergency visit is to bring the case under control by eliminating the patient’s primary cause of distress, which is most often pain with or without swelling. Definitions of what constitutes an endodontic emergency vary, but severe pain and swelling are the hallmarks of an emergency. A flare-up is often defined as severe pain and/or swelling after endodontic treatment requiring an unscheduled appointment and active treatment. Traumatic injuries may also be the cause of an emergency visit (see Chapter 11 ).
Learning Objectives
After reading this chapter, the student should be able to:
- 1.
Recognize the incidence of flare-ups.
- 2.
Describe appropriate diagnostic procedures for endodontic emergencies.
- 3.
Describe the initial patient contact and patient management issues.
- 4.
Describe the role of the staff in discriminating between a true emergency and a nonemergent case.
- 5.
Recognize the categories of flare-ups: pretreatment, intervisit, and postobturation.
- 6.
Describe appropriate nomenclature for diagnostic categories of pulpal and periapical pathologic conditions.
- 7.
Describe the causes of flare-ups and their management.
- 8.
Recognize anatomic factors that may lead to more rapid progression of infection.
- 9.
Recognize the importance of profound anesthesia.
- 10.
Describe the potential role of predisposing factors, including genetics, gender, and anxiety, in exacerbations.
- 11.
Use preoperative, intraoperative, and postoperative pharmaceuticals (e.g., anxiolytics, anesthetics, antiinflammatories, analgesics, and antimicrobials) in emergency cases.
Endodontic emergencies represent an important and complex part of clinical practice. Proper diagnosis and treatment require a knowledge of pulp and periapical pathosis and the ability to use the appropriate diagnostic tests. Diagnostic findings must be synthesized with the patient’s medical and dental history and chief complaint to select the best clinical procedures and therapeutics to address the emergency. The clinician must have an understanding of pain mechanisms, local anesthesia, the appropriate use of therapeutics, and patient management skills. Emergencies may occur prior to the inception of treatment, during treatment, or immediately after the canal or canals have been obturated. Clinical, biologic, and predisposing factors associated with flare-ups are reviewed in this chapter.
The immediate goal of an emergency visit is to bring the case under control by eliminating the patient’s primary cause of distress, which is most often pain with or without swelling. Definitions of what constitutes an endodontic emergency vary, but severe pain and swelling are the hallmarks of an emergency. A flare-up is often defined as severe pain and/or swelling after endodontic treatment requiring an unscheduled appointment and active treatment. Traumatic injuries may also be the cause of an emergency visit (see Chapter 11 ).
Diagnosis and Treatment Planning
Determining the cause of the pain and/or swelling is a critical initial step in the emergency visit. Without an accurate diagnosis, treatment is unlikely to be effective. Initially, the clinician must determine whether the cause of the problem is odontogenic or nonodontogenic. Determination of the precise cause of the emergency follows. A number of potential causes must be considered, including microbial, occlusal, psychogenic, or referred pain of dental or nondental origin. Often, simply listening to the history of the chief complaint and onset of the symptoms provides sufficient information for the clinician to make a tentative diagnosis, which must then be confirmed with radiographs and clinical tests.
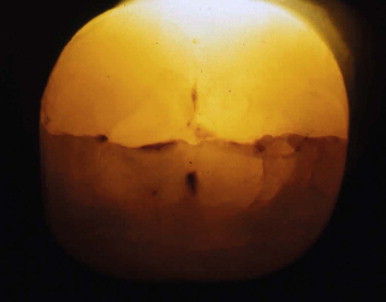
There are numerous classic patient narratives that provide critical information. An example is the patient who describes having had no pain until he or she bit down on something hard, which resulted in an immediate, sharp, lancinating pain and left a tooth tender to even finger pressure. Those few words are a powerful clue to causation and require investigation into a possible vertical or other type of fracture ( Fig. 10.1 ).
By contrast, a patient who relates being awakened by pain at night but then feeling better as the day progresses, only to have the pain return during sleep, does not fit the most common profile of an irreversible pulpitis. This patient requires a differential diagnosis for bruxism, temporomandibular joint dysfunction (TMD), or irreversible pulpitis.
The astute diagnostician must be a good listener and be able to synthesize information. Basic clinical tests include palpation, percussion, and thermal and electrical testing. Radiographs are an essential component of the diagnostic visit and may include periapicals, bitewings and cone beam computed tomography (CBCT). The clinician is cautioned against making a diagnosis based on a single radiograph (see Chapter 5 for further discussion of the diagnostic process).
Treatment planning involves a series of questions that must be answered prior to initiating treatment and may require consultation with the referring dentist and/or other health care professionals. Once the diagnosis has been made, an important question concerns the endodontic prognosis of the tooth. Factors include the restorability of the tooth, the crown-to-root ratio, the periodontal status, and the overall restorative plan, in addition to systemic health factors that could influence the plan. To determine an appropriate plan, additional information may be required from other dentists and physicians. The patient’s past dental history is also a factor. A patient missing numerous teeth and with poor oral hygiene is probably not the best candidate for an endodontic procedure with a questionable prognosis. A basic question to consider is how the patient’s oral health interests are best served. Should endodontic therapy be performed, or would an implant be a better approach? A review of the literature indicates that both procedures have a high rate of success when treatment is properly planned and completed.
Incidence of Exacerbations
The incidence of exacerbations has been estimated to be as low as 1.5% and as high as 20%. This wide range of estimates may be attributed to different definitions of exacerbations, varying study designs, and other procedural variations. A consistently high incidence of exacerbations should serve as a signal to the clinician to evaluate basic procedures, such as accuracy of measurement control and instrumentation. Breakdowns in either of those procedures could account for high rates of exacerbation.
The Initial Patient Contact
The initial emergency patient contact occurs most often by telephone prior to the initiation of endodontic treatment. The patient may report a history of long-term, low-level pain that has escalated to a more severe level. At this point the dentist must begin a basic triage, which includes determining whether the situation is truly an emergency and whether the problem seems to be odontogenic in nature. It may not be possible to clearly determine the status of the patient by telephone, and it is recommended that the clinician see such patients on an emergency basis to better determine the diagnosis and appropriate treatment.
The staff must be trained to respond appropriately to emergency calls. The person receiving the initial call should be able to differentiate between what is and is not a true emergency. However, when doubt exists about the urgency of the case, the clinician must make the final decision.
Patient Management
Patient anxiety is an important factor in achieving a satisfactory endodontic outcome, especially at an emergency visit. More than 200 studies indicate that preemptive behavioral intervention to reduce anxiety before and after surgery reduces postoperative pain intensity and intake of analgesics and accelerates recovery. A clinical study determined that the higher the level of anxiety, as measured by a visual analogue anxiety scale, the less likely it was that pain would be eliminated after administration of a local anesthetics. A conversation with the patient prior to treatment, in which the clinician discusses the pain-preventive strategy, including the use of profound local anesthesia, is an important element of the therapeutic approach.
Profound Anesthesia
Achieving profound local anesthesia for teeth with irreversible pulpitis is challenging and critical. Maxillary anesthesia is usually achieved by the use of infiltration or block anesthesia in the buccal and palatal areas. If profound anesthesia is defined as achieving the complete absence of pain, a single injection for a mandibular molar is usually insufficient. Intraosseous, ligamental, and intrapulpal injections are valuable supplementary injections that can help achieve this goal (see Chapter 9 ). It is important to note that a numb lip is not adequate proof of complete local anesthesia. The clinician is advised to recheck the chief complaint prior to initiating treatment. Absence of the chief complaint, whether it is thermal sensitivity or pain on percussion, is the best means of determining profound anesthesia.
Categories of Emergencies
Pretreatment Emergency
As mentioned, patients may present with a history of long-term, low-level discomfort that has suddenly escalated to intolerable pain and swelling. It is essential that a thorough diagnosis be made prior to instituting treatment. Usually, such emergencies are accompanied by a high level of patient anxiety, which can further complicate diagnosis and treatment. Teeth that cause pretreatment emergencies may be associated with irreversible pulpitis and/or symptomatic periodontitis or pulp necrosis with or without apical pathosis and swelling. Swelling may be localized or diffused. Each of these situations requires a somewhat different clinical approach based on biologic considerations.
Management of Irreversible Pulpitis
Basic biologic processes may explain the cause of an exacerbation of a tooth with irreversible pulpitis. Irreversible pulpitis is often the result of inflammation of the pulp due to a microbial insult from caries or microleakage associated with a defective restoration. Exacerbation of a tooth with irreversible pulpitis is characterized by pain, which may be severe. The pain may occur with or without provocation and tends to increase in severity. A pulp with irreversible pulpitis is usually free of bacterial colonization in the root canal. Infection is most often confined to the coronal site of the pulp that is exposed to the oral cavity. As long as the radicular pulp remains vital, it usually protects itself against microbial invasion and colonization.
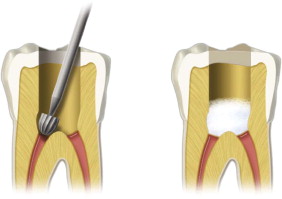
It has been demonstrated that removal of the pulp from the pulp chamber (pulpotomy) is a highly predictable approach to alleviating pain at an emergency visit ( Fig. 10.2 ). It is considered preferable, if time permits, after measurement control, to remove all pulp tissue from the canal or canals. A clinical study demonstrated that partial pulpectomy resulted in a higher rate of postoperative pain (13%) compared with pulpotomy (6%). Other important factors associated with postoperative pain were female gender, younger age, and molar teeth. An emergency was defined as a visit to the dental emergency clinic within 24 hours of treatment for pain not controlled by ibuprofen, aspirin (ASA), or Tylenol. It is challenging to remove inflamed tissue and infected debris from the canal system without pushing toxic material through the apical foramina into the periapical tissues. Establishing an accurate measurement control and maintaining it during instrumentation are critical in avoiding this complication.
Interappointment Emergencies
Causes of Flare-Up
There are a number of hypotheses concerning the true cause of flare-ups, which have been described as multifactorial. Causes include iatrogenic mechanical irritation of the tissues beyond the apical terminus and/or the pushing of dentin chips and remnants of infected pulp tissue into the periapical tissues. A procedural accident often impedes therapy or makes it impossible for therapy to be completed, such as by preventing thorough mechanical debridement or creating a bacteria-tight seal for a root canal system. An increased risk exists when a procedural accident occurs during treatment of infected teeth. There are also chemical factors, including irrigants, intracanal dressings, and sealers. Endodontic procedural errors are not the direct cause of treatment failure; they increase the risk of failure because of the clinician’s inability to eliminate microorganisms from the infected root canals.
The number of treatment visits has also been examined as a factor in flare-ups. In a retrospective study, the flare-up rate in necrotic molars in one-visit compared with two-visit endodontic treatment was examined. Treatment records of 402 consecutive patients with pulpally necrotic first and second molars were compared. One-visit treatment showed an advantage at the 95% confidence level. However, retrospective analyses do not control for the reason that a case took one or more appointments to complete, and some other studies have shown no differences between single and multiple visits in the incidence of flare-ups.
Interappointment flare-ups most often occur after instrumentation of the canal system. The biologic factors resulting in pain in cases with irreversible pulpitis (vital cases) and in pain/swelling in necrotic (nonvital) cases may differ and are reviewed.
Frequently, iatrogenic errors cause problems. An example is leaving shredded pulp tissue in the canal system. After a working length measurement has been taken, the clinician should follow with complete debridement of tissue from the canal. This does not mean that the canal is fully shaped and ready for obturation, but rather that all pulp tissue in the canal has been removed.
Most important, before emergency treatment is initiated, the clinician should understand the biologic cause of the problem. For example, was there an iatrogenic component to the exacerbation, as occurs when an inaccurate measurement is used, or was an accurate measurement established but not maintained? Another reasonable possibility concerns the tooth’s occlusion. Was the tooth under treatment left high in occlusion? This would exacerbate an inflamed periodontal membrane, resulting in pericementitis.
It has been determined that clean dentin chips pushed into the apical tissue did not result in a vigorous tissue reaction, whereas dentin chips contaminated by bacterial debris posed a problem and resulted in an inflammatory reaction. In a nonvital case (necrotic, infected), debris may have been pushed into the periapical tissues, resulting in an immunologic and inflammatory response. These possibilities and others must be considered before selecting the appropriate treatment and determining whether an analgesic and/or an antibiotic are indicated. It is important to note that an antibiotic should never be used to control pain in a case with irreversible pulpitis.
Biology of the Necrotic (Nonvital) Exacerbation
If we consider treatment of irreversible pulpitis (vital case) to be essentially a biologic challenge of removing well-innervated and inflamed tissue from a canal without causing increased pain, the necrotic (nonvital) case may be considered a microbiologic problem. Microorganisms are the most common etiologic cause of postoperative pain and post-treatment disease in the necrotic case. Exacerbation of the necrotic tooth occurs in the periapical tissues and is an immune/inflammatory reaction due to the extrusion of intracanal bacteria and tissue debris. The exacerbation may be characterized by pain with or without swelling. Swelling may be diffused or localized or may become a cellulitis.
As noted previously, clean dentin chips pushed into the apical tissue did not result in a tissue reaction, whereas those contaminated by bacterial debris resulted in an inflammatory reaction.
Treatment of the necrotic exacerbation is focused on the root canal if there is no swelling. Reinstrumentation and irrigation are the basic treatments directed at reducing the intracanal level of microorganisms. If swelling exists, the clinician should consider incision and drainage followed by instrumentation and irrigation of the canal. Antibiotics alone should not be used without concomitant instrumentation and irrigation. Although incision and drainage is directed at reducing periapical tissue pressure and eliminating pus, reinstrumentation and irrigation are directed at the primary cause of the problem, which is remaining intracanal bacteria.
Postobturation Emergencies
It has been demonstrated histologically that the most favorable response of periapical tissues occurred when both instrumentation and filling were short of the apical constriction. A clinical study found that the best treatment outcome in infected teeth with periradicular lesions occurred when the apical terminus of the filling was 0 to 2 mm short of the radiographic apex. The same study determined that the prognosis was less favorable with significant underfill or overfill. These findings are corroborated by other research reports.
Postobturation emergencies may include pain and diffuse swelling. Tenderness to finger pressure or percussion or an inability to comfortably bite on the tooth is often a predictor of postobturation pain. It is strongly recommended that obturation be deferred in such cases until the patient is pain free and the tooth in question can be used in function. During treatment of a postobturation exacerbation, the clinician must decide whether it is necessary to remove the root canal filling. Much depends on the condition of the tooth prior to obturation. A critical factor is the status of the tooth prior to filling. Was the tooth asymptomatic or did symptoms persist after instrumentation? Filling canals in the presence of continuing symptoms is often a predictor of postobturation complications. The nature of the swelling should also be considered. If there is swelling, is it diffuse in nature or becoming larger and fluctuant? Treatment for postobturation exacerbations may range from using pharmacotherapeutics, including analgesics and/or antibiotics, up to retreatment with or without incision for drainage. The clinician must consider the variables and then determine whether the primary cause of the patient’s symptoms is inflammatory in nature, due to the procedure itself, or active infection. In most cases, if basic endodontic principles have been followed, the root canal filling does not have to be removed and postobturation pain can be treated with analgesics.
Predisposing Factors
An increasing body of evidence indicates that there may be factors that predispose a patient to pain and that could affect the outcome of treatment. Among those factors are the patient’s genetics, gender, and level of anxiety.
Genetics
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


