Introduction
Severe crowding can be treated with serial extraction (SE) in the mixed dentition or with late premolar extraction (LPE) in the permanent dentition. The aim of this study was to investigate the efficiency of orthodontic treatment in SE patients and LPE patients.
Methods
Retrospective chart review identified 51 SE patients and 49 LPE patients treated with fixed appliances. Number of appointments, length of time, and estimated total chair time were determined prior to the placement of fixed appliances and during fixed appliance treatment. Peer assessment rating (PAR) scores were obtained at T1 (start of fixed appliances) and T2 (removal of fixed appliances) for both groups, and at T0 (prior to extraction of the first premolars) for the SE group.
Results
The mean T1 PAR score for SE patients was significantly lower than LPE patients ( P <0.001); mean T2 PAR scores were not significantly different ( P = 0.27). Active treatment time (T1 to T2) was significantly ( P <0.001) less for SE patients than LPE patients. Total time (T0 to T2) and total number of appointments were significantly greater for the SE group compared with the LPEgroup ( P <0.001).
Conclusions
SE and LPEresulted in similar final occlusal outcomes. SEs might reduce active treatment time, but significant observation time precedes active treatment.
Severe crowding may be treated early with serial extraction (SE) in the mixed dentition or with late premolar extractions in the permanent dentition. The goal of SE is to create space in the mixed dentition for the eruption of permanent teeth into more favorable positions over basal bone to prevent or reduce the complexity of future orthodontic treatment in the permanent dentition. The majority of SE patients, however, require comprehensive fixed orthodontic treatment, as tipping, residual spacing, and alignment problems commonly occur with the eruption of the remaining permanent teeth. An alternative approach is to intervene with late premolar extractions (LPEs) when eruption of the permanent dentition is complete and crowding has developed, which will universally require comprehensive orthodontic treatment to align the remaining teeth and close residual extraction spaces. Suggested benefits of SE over LPE have included a shortened treatment time and associated economic savings.
The classic serial eruption sequence starts with the extraction of the primary canines, which facilitates the alignment of the permanent incisors. The primary first molars are then extracted to ensure the first premolar erupts earlier than the permanent canine. The first premolars are extracted soon after eruption to allow space for favorable eruption of the canine. This sequence may require modification when at the time of extraction of the first primary molar, the canine appears to be erupting before the first premolar. In these cases, the first primary molar can be extracted and the first premolar enucleated at the same appointment. This modification is most often indicated in the mandibular arch and may save the patient an additional surgical procedure.
Previous comparisons of SE and LPE have focused on the long-term stability of treatment results and treatment time in fixed appliances. However, overall treatment time, which includes any prefixed appliance therapy, was not considered in these investigations. Only 1 study has included the period prior to fixed appliances in an analysis of treatment outcomes and the duration of treatment. This study had a small sample size of 20 patients per treatment group and did not compare the occlusal status of the SE and LPE groups immediately prior to the start of fixed appliance treatment.
The aim of this study was to compare the efficiency of orthodontic treatment for SE and LPE cases between 3 time points: initial contact with the orthodontic practice, start of fixed appliance therapy, and completion of appliance therapy. Variables included number of appointments, treatment time, and estimated total chair time. Another aim was to investigate the occlusal status of the SE and LPE patients at the initiation and completion of fixed appliance therapy.
Material and methods
This retrospective study was reviewed and approved by a biomedical institutional review board. All potential SE and LPE patients in a 2-doctor 3-office private practice were initially identified using treatment summary records maintained by the orthodontists. Treatment records for all initially identified SE and LPE patients consecutively treated with fixed appliances between January 1, 1990 and March 31, 2006 were then screened using general inclusion criteria to identify potentially eligible SE and LPE cases.
The 2 orthodontists planned treatment jointly in all the cases in each of the 3 offices during the first 2 years of the time period and used consistent treatment planning criteria to plan extractions for all patients. In the SE and LPE cases, no mixed dentition analysis or arch length analysis done by measuring tooth size and arch length was performed prior to the ordering of extractions. However, a formalized set of criteria was used by the practitioners to determine suitability for extractions. Patients who received SEs were estimated to have more than 8 mm of crowding by visual examination. Patients with severe anterior-posterior discrepancies, incisor protrusion, decreased vertical face heights, and excessive deep bites were not considered suitable candidates for the SE group. In the LPE patients, crowding was also estimated by visual examination. Severe crowding along with incisor protrusion, lip protrusion, lip incompetence, a deep curve of Spee, and future incisor instability were used as justification for pursuing extraction treatment in the LPE group. The practitioners prescribed SE if subjects had significant crowding and were referred to the practice while in the mixed dentition period. Patients who were referred to the practice with severe crowding of the permanent dentition were prescribed LPE.
Each SE patient received an extraction sequence based on an assessment of their individual treatment needs, eruption sequence, and tooth development. The office protocol was to first extract the primary canines. The first premolar was extracted next, if the eruption sequence was deemed to be first premolar, canine, second premolar. If the eruption sequence was canine, first premolar, second premolar, the primary first molar was extracted, and the first premolar was enucleated at the same appointment. This approach was used to reduce the number of surgical interventions, some of which required sedation for behavior management.
The general inclusion criteria were extraction of 4 permanent teeth, 1 in each quadrant, completion of comprehensive fixed appliance treatment after extractions, and availability of pre- and posttreatment records. The general exclusion criteria were more than 1 tooth in posterior cross bite, angle Class II molar relationship beyond 1/2 cusp Class II, angle Class III molar relationship beyond ¼ cusp Class III, 21 years or older, missing teeth (other than third molars), previous orthodontic treatment, incomplete records, and active phase I orthodontic tooth movement (passive Nance arches and lower lingual holding arches were acceptable).
Subjects were included in the SE group if a minimum of 1 year of physiologic drift occurred after extractions. Subjects were included in the LPE group if extractions occurred after the permanent dentition was partially or fully erupted, and fixed appliances were placed no longer than 3 months after extractions. Using these criteria, 51 SE and 49 LPE patients were identified.
Subjects in the 2 treatment groups were not matched on initial malocclusion or crowding. The LPE group did not have initial records (T0) taken at the same age in the mixed dentition period as the SE group. By the beginning of fixed appliance treatment, subjects in the SE group had already had extractions and drifting of teeth, while the LPE group had not yet received any treatment.
Data collection and measures
Records examined included the complete treatment chart as well as plaster models and panoramic radiographs taken at the following times: prior to the extraction or enucleation of first premolars (T0) (SE), prior to the initiation of fixed orthodontic treatment (T1) (SE and LPE), and after completion of fixed orthodontic treatment (T2) (SE and LPE). The orthodontic offices used paper treatment charts and also maintained treatment summary records that allowed the initial identification of all patients treated with SE and LPE. Records of these initially identified patients were then screened by 1 examiner using the inclusion and exclusion criteria. The following information was recorded for each SE and LPE patient who met the inclusion criteria: date of birth, date of each orthodontic visit, length (minutes) of chair time scheduled for each orthodontic visit, type of procedure scheduled at each orthodontic visit, and tooth extraction referrals written, if any, at each visit. The estimated chair time for each orthodontic visit was based on the office computer scheduling system. This may not be representative of the total orthodontist time spent with a patient but does give an estimation of how much time was required to prepare the chair for the patient, seat the patient, complete the assessment, and dismiss the patient. Regardless of whether the patient was in active treatment or an SE observation, actual office chair time was required to accommodate patients at each visit.
Panoramic radiographs taken at T0 for SE and at T1 for LPE were examined to determine the presence of all permanent teeth except third molars and verify the suitability of the extraction treatment plan. Dental age at T1 was determined (Demirjian et al ) to compare dental ages of the 2 groups. All scoring of films was done by a single examiner. Thirteen panoramic films were chosen randomly for remeasurement to test for intraexaminer reliability for dental age determination.
Peer assessment rating (PAR) index scores were calculated for SE models at T0, T1, and T2 and for LPE models at T1 and T2. All measurements were made by 1 examiner, who was trained and calibrated using a PAR reliability training set of dental casts. Intraexaminer reliability was determined using 38 randomly selected dental casts from the study for remeasurement. Anterior component and total PAR index scores were calculated using a weighting system developed by Richmond et al.
Statistical analyses
Unpaired t tests for anterior component and total PAR scores and Wilcoxon rank sum tests for the length of time measures were used to compare the 2 treatment groups. For analysis of categorical data, a Fisher exact test was used. Intraexaminer reliability was assessed using intraclass correlation. Bivariate association between length of treatment time variables and total PAR scores was assessed using a Spearman correlation. Analysis of covariance (ANCOVA) was used to compare the length of treatment times in the 2 treatment groups after adjusting for the T1 PAR score. Median values and quartiles were used to summarize length of time measures (number of months of pre–active treatment and active treatment, number of visits to the orthodontist, and minutes of chair time) because of the skewed distributions of the measures and to give a better representation of the central tendencies of these variables. Braces free months was defined as the difference between the median active treatment time for the LPE group and the active treatment time for each SE patient. The level of significance was set at P = 0.05 for all analyses.
Results
Description of sample
The demographic characteristics of the 2 treatment groups are given in Table I . The study group consisted of 51 SE patients (19 males and 32 females) and 49 LPE patients (19 males and 30 females).
| Males | Females | Chronological age (years) | Dental age (years) | |||
|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T1 | |||
| SE | 19 | 32 | 7.95 (0.92) | 13.11 (0.92) | 14.89 (0.95) | 14.02 ∗ (0.99) |
| LPE | 19 | 30 | — | 13.41 (2.03) | 15.52 (2.01) | 13.97 ∗ (1.56) |
The intraexaminer reliability for total PAR calculated from the training set was ICC = 0.92 and from the repeated measure of study casts was ICC = 0.99. No systematic difference in the replication of PAR scoring occurred ( P = 0.49). Intraexaminer reliability for measurement of dental age yielded an ICC = 1.0.
There was no significant difference ( P = 0.84) in dental age at T1 between SE and LPE groups, which indicated that the effect of dental development on treatment time for the fixed orthodontic treatment would be similar between the groups.
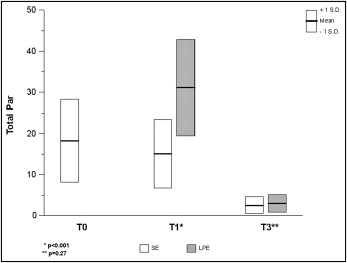
The average anterior component PAR scores for both the upper and lower arch and the total PAR score were significantly different for the SE and LPE groups at T1, with the LPE group, on average, having higher PAR scores ( Fig 1 , Table II ), which indicates that the SE group had early alignment of the anterior teeth. The extraction of the premolars allowed incisor alignment to improve before fixed appliances were placed. At T2, the average anterior component PAR scores for the upper and lower arches and the total PAR scores were not significantly different ( Table II ), which suggests that the final occlusal outcomes were similar for the 2 groups.
| Time | PAR Index | SE | LPE | P value |
|---|---|---|---|---|
| T0 | Total PAR | |||
| Mean | 18.24 | n/a | ||
| SD | 10.09 | n/a | ||
| Maxillary anterior PAR | ||||
| Mean | 5.20 | n/a | ||
| SD | 4.01 | n/a | ||
| Mandibular anterior PAR | ||||
| Mean | 2.24 | n/a | ||
| SD | 2.64 | n/a | ||
| T1 | Total PAR | |||
| Mean | 15.18 | 31.27 | <0.001 | |
| SD | 8.35 | 11.68 | ||
| Maxillary anterior PAR | ||||
| Mean | 3.49 | 5.49 | <0.001 | |
| SD | 2.60 | 3.38 | ||
| Mandibular anterior PAR | ||||
| Mean | 1.27 | 4.84 | <0.001 | |
| SD | 1.59 | 2.50 | ||
| T2 | Total PAR | |||
| Mean | 2.61 | 3.08 | 0.27 | |
| SD | 2.05 | 2.18 | ||
| Maxillary anterior PAR | ||||
| Mean | 0.14 | 0.12 | 0.84 | |
| SD | 0.40 | 0.33 | ||
| Mandibular anterior PAR | ||||
| Mean | 0.07 | 0.06 | 0.74 | |
| SD | 0.27 | 0.24 |
Using previously defined criteria for absolute final PAR scores (Richmond et al and Tulloch et al ) the vast majority of patients in the SE (94%) and LPE (90%) groups had a final total PAR score of 5 or less, placing them in the “almost ideal” occlusion category. In both groups, the remainder of the patients had a PAR score between 6 and 10, which placed them in the “acceptable occlusion” category. No patient in either group finished in the “less than acceptable” occlusion category with a PAR score more than 10. The distribution of these categories for total PAR score at T2 were not statistically significant different between the treatment groups ( P = 0.48).
Table III presents the length of treatment time measures (months of treatment, numbers of visits, and minutes of chair time) for each group for the total treatment time as well as active fixed appliance treatment time. The SE group had a significantly longer average total treatment time ( P <0.001) and significantly more total number of visits than the LPE group ( P <0.05). The LPE group had a significantly longer average active treatment time, more active treatment visits and more active treatment chair time than the SE group ( P <0.001). However, the total treatment chair time in minutes, on average, was not significantly different between the groups ( P = 0.07).


