Introduction
There is a popular belief among some musicians that playing a wind instrument regularly can affect the position of the teeth. The aim of this study was to investigate this hypothesis.
Methods
A cross-sectional observational study was carried out, comparing the occlusions of 170 professional musicians selected from 21 orchestras and organizations in the United Kingdom. The subjects were subdivided according to type of instrument mouthpiece and included 32 brass players with large cup-shaped mouthpieces, 42 brass players with small cup-shaped mouthpieces, and 37 woodwind players with single-reed mouthpieces. Fifty-nine string and percussion players formed the control group. Impressions were taken of the teeth of each subject, and occlusal parameters were assessed from the study casts. The results were analyzed by using analysis of variance (ANOVA) and chi-square tests.
Results
No statistically significant differences were found in overjet ( P = 0.75), overbite ( P = 0.55), crowding (maxillary arch, P = 0.31; mandibular arch, P = 0.10), irregularity index (maxillary arch, P = 0.99; mandibular arch, P = 0.16), and the prevalence of incisor classification ( P = 0.15) between the wind instrument players and the control group. However, the large-mouthpiece brass group had a significantly higher prevalence of lingual crossbites in comparison with all other groups.
Conclusions
Playing a wind instrument does not significantly influence the position of the anterior teeth and is not a major etiologic factor in the development of a malocclusion. However, playing a brass instrument with a large cup-shaped mouthpiece might predispose a musician to develop lingual crossbites or lingual crossbite tendencies.
A popular belief among wind instrument players and their teachers is that playing a wind instrument can lead to the development of malocclusion. Patients and their parents often ask dentists and orthodontists whether playing a wind instrument can affect the position of teeth or whether the patient’s malocclusion is due to regular wind instrument playing. A review of the literature showed no clear agreement in this area. As a result, it has been impossible to advise patients with any certainty about the potential effects of playing a wind instrument on the occlusion.
According to Proffit’s equilibrium theory, the position of the teeth depends on forces exerted from the tongue and lips, forces from the dental occlusion, forces from the periodontal membrane, and habits such as thumb sucking. The effects of digit and thumb sucking on the occlusion are well documented in the medical literature. Tooth movement requires the application of force exceeding a minimum threshold of magnitude and duration. On a theoretical basis, playing a wind instrument might exert external forces to the occlusion in a similar manner as thumb sucking, and hence might result in the development of malocclusion. The pressure exerted by brass instruments on the teeth has been documented to be as high as, or even higher than, thumb sucking. In addition, there is little evidence regarding the optimum magnitude of force, and various animal studies have shown that a force duration of as little as 8 hours a day results in tooth movement.
A substantial part of the literature on the effects of playing a wind instrument on the occlusion comprises expert opinions and anecdotal evidence based on anatomic assumptions and logic rather than on evidence-based research.
Strayer, a professional bassoonist and orthodontist, was the first author to propose, based on observation, that playing a wind instrument can affect the position of the teeth and therefore cause or correct a malocclusion. He classified wind instruments into classes A, B, C, and D and suggested that the effects of playing a wind instrument on the position of the teeth might vary according to the type of mouthpiece and embouchure that is involved ( Fig 1 ). In the literature, other authors (Porter and Dunn ) have since supported Strayer’s observations and proposed similar theories.
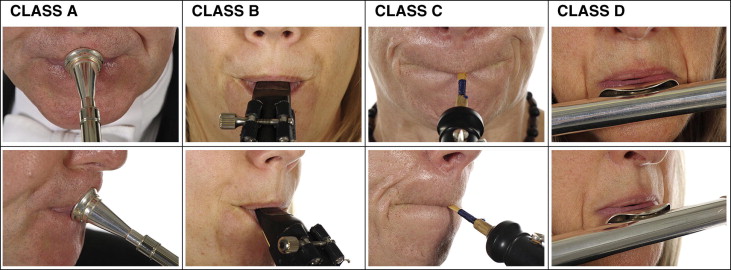
It therefore seems possible to theorize, based on observation of the embouchure ( Fig 1 ), that forces distributed around the dentition when playing instruments could have the following effects for different classes of instruments.
Class A instruments can exert a horizontal force on the maxillary and mandibular incisors that might result in retroclination of maxillary and mandibular incisors and lead to a reduction in overjet and an increase in overbite.
Class B instruments can exert horizontal and vertical forces on the maxillary and mandibular incisors that might result in maxillary incisor proclination, mandibular incisor retroclination, intrusion of maxillary and mandibular incisors, and therefore an increase in overjet and a reduction in overbite.
Class C instruments can exert horizontal and vertical forces on the maxillary and mandibular incisors that might result in retroclination and intrusion of maxillary and mandibular incisors and therefore a reduction in overjet and overbite.
Class D instruments can exert a horizontal force on the mandibular incisors that might result in retroclination of mandibular incisors and therefore an increase in overjet.
Since the early observational evidence, numerous authors have attempted to examine over the last 3 decades the effects of playing a wind instrument on the occlusion more rigorously. The majority of the published studies have been cross-sectional observational studies comparing the study casts or the lateral cephalograms of wind instrument players with those of a control group. Parker and Rindisbacher concluded that playing a wind instrument has little, if any, effect on the occlusion. On the contrary, Pang, Gualtieri, and Brattström et al concluded that playing a wind instrument might affect the inclination of the maxillary and mandibular incisors and therefore result in an increase or a decrease in overjet or overbite.
In the context of currently accepted optimum research practice, many of the previously reported studies might be considered to suffer from flaws that could affect the validity of their conclusions. For example, potential inaccuracies might have arisen because of a small sample size, the lack of a control group, or a biased control group such as one comprising dental students or student dental assistants, or the inclusion of amateur players, children and adolescents, subjects who had previously undergone orthodontic treatment, and subjects from various ethnic groups. Furthermore, in these studies, the wind instrument players were often not separated into groups or classes according to the type of instrument or the shape of the mouthpiece, study casts were not usually taken, the examiners were rarely blinded, and the participants’ dental statuses were commonly not stated.
This study was devised to help provide evidence-based advice on whether playing a wind instrument affects the position of teeth or whether it is a causative factor in the development of malocclusion. Our aim was to assess whether playing a wind instrument has an effect on the position of the teeth or causes a malocclusion. In particular, the objectives of this study were to:
- 1.
Determine if playing a wind instrument affects overjet, overbite, or the transverse molar relationship.
- 2.
Determine if playing a wind instrument causes crowding, irregularity, or alters the intermolar widths.
- 3.
Determine if there is a difference in the prevalence of the incisor relationship and crossbites in brass and woodwind players when compared with musicians who do not play a wind instrument.
The null hypothesis was that there is no difference in the occlusions of professional wind instrument players when compared with a control group of musicians who do not play wind instruments.
Material and methods
Independent-group t test analysis estimated that 32 subjects per group were required to detect a difference of 2 mm in overjet among the various groups. This was based on an alpha significance level of 0.05 with 95% power. The standard deviation for the sample size was calculated as 1.9 mm based on data from the National Health and Nutrition Examination Survey III, which included detailed data on overjet across a large population of white subjects.
Ethical approval was obtained from the University of Birmingham Research and Ethics Committee and the Royal Northern College of Music Research and Ethics Committee in the United Kingdom. All subjects were treated according to the Declaration of Helsinki (1964) and the British Psychological Society’s code of ethics and conduct (2006). Signed informed consent was obtained from each subject who participated in the study.
Various well-established and reputable professional orchestras, jazz bands, and music colleges were contacted. The subjects comprised wind instrument players of classes A and B (Strayer’s classifications), and the control group comprised string instrument and percussion players, recruited from the same organizations.
The subjects were therefore separated into 4 groups: (1) players of large-mouthpiece brass instruments, such as the tuba and trombone; (2) players of small-mouthpiece brass instruments, such as the trumpet and French horn; (3) players of single-reed instruments such as the clarinet and saxophone; and (4) players of string and percussion instruments (control group).
The subjects were selected from the following organizations: Royal Philharmonic Orchestra, City of Birmingham Symphony Orchestra, London Philharmonic Orchestra, Lucerne Symphony Orchestra, Oxford Philomusica, Royal Liverpool Philharmonic Orchestra, BBC Big Band, Welsh National Opera Orchestra, Halle, BBC Philharmonic Orchestra, Opera North, National Saxophone Choir, Clarinet and Saxophone Society, Trinity College of Music, BBC Scottish Orchestra, Royal National Scottish Orchestra, Royal Scottish Academy of Music and Drama, BBC Concert Orchestra, and Royal Welsh College of Music and Drama. Furthermore, 2 organizations, the East London Clarinet Choir and the Notebenders Jazz Club, were visited, but no musician satisfied the selection criteria.
The included subjects were white men and women who were professional wind instrument players, practiced on average at least 3 hours daily, and for at least the last 4 years, and started playing a wind instrument before they were 14 years old. The control group comprised professional string and percussion players from the same orchestras and organizations as the wind instrument players.
Wind instrument players who played more than 1 class of wind instruments either professionally or recreationally, with the exception of single-reed players who also played the flute or the piccolo, were excluded. String and percussion players who played or used to play a wind instrument recreationally were excluded.
In terms of their dental status, we excluded subjects (wind, string, and percussion players) who had previously undergone orthodontic treatment; had extractions of permanent teeth other than second and third molars; had retained deciduous teeth or supernumerary teeth, crowns on permanent teeth other than first, second, and third molars; had restorations on incisors and canines that extended over 2 surfaces; or had pathology, including periodontal disease, previous fractures of the maxilla or the mandible, and dental cysts. Subjects who admitted to a digit-sucking habit that persisted until the age of at least 10 years and subjects who smoked a pipe were also excluded.
The musicians who satisfied the criteria on the basis of written questionnaires had a brief examination of their teeth. Those who were eligible to participate on the basis of the inclusion and exclusion criteria had impressions taken at their practice venues. Study casts were made and coded to preserve anonymity and ensure that there was no observer bias during their assessment.
Recruitment of participants stopped as soon as 32 musicians were obtained for each group, as dictated by the sample size calculation. A total of 170 musicians participated in the study. They comprised 32 subjects in the large-cup brass group, 42 subjects in the small-cup brass group, 37 subjects in the single-reed group, and 59 subjects in the control group. Inclusion of more than 32 subjects in the first 3 groups increased the statistical power of the study.
The following features were assessed on the study casts: (1) overjet (mm), (2) overbite (mm), (3) British Standards Institute incisor relationship, (4) maxillary and mandibular intermolar widths (mm), (5) crowding in the maxillary and mandibular labial segments (mm), (6) Little’s irregularity index (mm), and (7) crossbites, with reference to the maxillary first permanent molars.
All measurements were made by 1 examiner (E.G.). Digital calipers were used to measure linear measurements such as the overbite, intermolar width, and crowding. The digital calipers were calibrated to ensure accuracy on every 12 successive study casts.
Incisor relationship was assessed according to the British Standards Institute incisor classification. This classifies incisor relationships as follows.
Class I, the mandibular incisor edges occlude with or lie immediately below the cingulum plateau of the maxillary central incisors.
Class II, the mandibular incisor edges lie posterior to the cingulum plateau of the maxillary incisors. There are 2 divisions. In Division 1, there is an increase in overjet and the maxillary central incisors are usually proclined. In Division 2, the maxillary central incisors are retroclined. The overjet is usually minimal but might be increased.
Class III, the mandibular incisor edges lie anterior to the cingulum plateau of the maxillary incisors. The overjet is reduced or reversed.
To define the intermolar widths, the mesiobuccal cusps of the maxillary and mandibular first molars were taken as reference points. Little’s irregularity index, which is the sum of the contact point displacements in the 6 anterior teeth, was measured as described by Little.
On each pair of casts, the presence or absence of a transverse discrepancy of tooth relationship (crossbite) was scored as follows.
- 1.
Absence of crossbite was defined when the palatal cusps of all maxillary molars occluded to the midpoint of the central fossa of the mandibular molars.
- 2.
Presence of lingual crossbites or lingual crossbite tendencies: a lingual crossbite tendency was defined when the palatal cusp of the maxillary first permanent molar occluded lingually to the central fossa of the mandibular first permanent molar. Lingual crossbite was defined when there was cusp-to-cusp contact or more.
- 3.
Presence of buccal crossbites or buccal crossbite tendencies: a buccal crossbite tendency was defined when the palatal cusp of the maxillary first permanent molar occluded buccally to the central fossa of the mandibular first permanent molar. Buccal crossbite was defined when the palatal cusp of the maxillary first permanent molar occluded on the buccal cusps of the mandibular first permanent molar.
The descriptions and definitions of crossbites of American orthodontists are the opposite of the description of the British Standards Institute classification that defines a buccal crossbite as a transverse discrepancy in tooth relationship where the buccal cusps of the mandibular teeth occlude laterally to the buccal cusps of the maxillary teeth.
Before taking the measurements, the reproducibility of the measurements was confirmed with a matched pairs t test by remeasuring 20 randomly selected study casts 9 days later. This confirmed that there was no significant difference between initial and subsequent measurements.
One-way analysis of variance (ANOVA) was used to compare the means of interval variables among the groups: overjet, overbite, crowding, Little’s irregularity index, and intermolar widths. The chi-square test was used to assess whether there was a difference in categorical variables among the groups: the proportions of subjects with various incisor classifications and crossbites. A retrospective sample size calculation, with the standard deviation calculated from the data of the subjects of this study, confirmed that there was 83% to 98% power for the analysis and comparison of all the other occlusal features.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


