Introduction
The aim of this study was to evaluate morphologically the effect of teriparatide on induced orthodontic movement of the maxillary first molars in ovariectomized rats.
Methods
Ovariectomized Wistar rats (n = 16), ovariectomized rats treated with teriparatide (n = 16), and nonovariectomized rats (n = 16) had orthodontic tooth movement for 5 and 7 days. The group treated with teriparatide received a subcutaneous injection (Forteo, Eli Lilly, Indianapolis, Ind; 30 μg/kg/day) for 90 days after the ovariectomy. Histologic sections obtained from the maxilla were prepared for the morphometric analysis of dental movement, the thickness of the periodontal ligament, and the number of osteoclasts in the pressure and tension areas of the apex of the root and alveolar crest in the distal root of the maxillary first molars.
Results
The ovariectomized rats treated with teriparatide had similar responses at 5 and 7 days after the induced dental movements compared with the untreated ovariectomized group. Both ovariectomized groups had greater molar movement on day 7 day compared with the controls ( P <0.05). There were no statistically significant differences between groups in the spacing of the periodontal ligament or the number of osteoclasts in the areas studied.
Conclusions
These data suggest that the treatment of osteoporosis with teriparatide is a good alternative for patients undergoing orthodontic treatment.
Bone remodeling is regulated by systemic hormones and local factors that affect the osteoblast cell line and exercise an effect on the replication of nondifferentiated cells as well as the recruitment and differentiated functions of the cells. This physiologic bone response comprises the basis of orthodontic treatment, in which dental movement is enabled by the processes of bone resorption and neoformation. Induced dental movement is not an exclusively mechanical event. It involves a sequence of biologic changes stemming from the action of cells in the periodontal ligament (PDL), which undergoes changes caused by the force exercised, thereby releasing chemical mediators that stimulate frontal bone resorption, causing movement of the tooth in the alveolus. Dissipation of the applied force then occurs, and the stimuli of mechanical stress and inflammatory response cease.
The effects of estrogen on bone tissue have been investigated with a wide range of methodologies. Although it is not completely understood, estrogen appears to involve a direct action on osteoblasts as well as an indirect action regulating other hormones. Ovariectomy leads to deficiency in the production of estrogen and causes clinical effects that are similar to menopause. With time, there is a reduction in bone mineral density, known as osteoporosis.
The pathogenesis of osteoporosis remains controversial and even obscure under certain aspects. However, estrogen deficiency in women and androgen deficiency in men are significant aspects in the development of this condition, even though the mechanisms involved are yet unknown. Estrogen is believed to stimulate osteoblasts. However, once osteoporosis has set in, steroids cannot reverse this condition. The involvement of parathormone, vitamin D, disorders in the absorption of intestinal calcium, or calcitonin is also postulated. Normal estrogen levels protect the skeleton from the action of parathormone by impeding the increase in osteoclast activity. The supplemental intake of calcium is beneficial in the prevention of osteoporosis. Dietary supplementation of vitamin D, however, has not demonstrated significant benefits.
In recent years, orthodontic treatment has become more accessible to the general public, and the increase in longevity has led to an increased demand for orthodontic treatment among adults. The aging process has led to greater numbers of patients with systemic diseases in orthodontic clinics, including those with osteoporosis. This disease can also cause changes in the maxillary bone tissue involved in orthodontic movement of the teeth.
Currently, the most common treatment for osteoporosis is the administration of bisphosphonate derivatives, which promote the recovery of mineral density by an inhibitory effect on osteoclasts. Thus, the remodeling process is normalized because of a reduction in osteoclast activity, with no direct effect on neoformation. However, it has been demonstrated that patients taking bisphosphonates for a long time can have less dental movement, thereby hampering orthodontic treatment.
Teriparatide (Forteo, Eli Lilly, Indianapolis, Ind) is a portion of the human parathyroid hormone (PTH), which is the primary regulator of calcium and phosphate metabolism in bones. Teriparatide is a new medication alternative for the treatment of osteoporosis; it promotes an increase in bone mineral density by stimulating osteoblasts, with no expressive interference in osteoclast activity. However, as yet, no studies have assessed the effects of this medication on dental movement. Thus, the purpose of this study was to analyze the relationship between induced orthodontic movement and therapy with teriparatide in ovariectomized rats.
Material and methods
All procedures involving animals received approval from the Ethics Committee on Animal Experimentation of the Universidade Estadual de Maringá in Brazil (process number 052/2006). Forty-eight Wistar rats ( Rattus norvegicus ) at 8 weeks of age were divided into 3 groups, anesthetized with an intramuscular injection of xylazine (0.1 mL/100 g) and ketamine (0.1 mL/100 g) and received bilateral laparotomy and ovary removal: group 1 (n = 16), ovariectomized rats; group 2 (n = 16), ovariectomized rats treated with teriparatide; and group 3 (n = 16), sham operated rats (control). The day after surgery and over the subsequent 90 days, the animals in group 2 received a subcutaneous injection of teriparatide (Forteo, 30 μg/kg/day). Throughout the experiment, all animals were kept in a bioterium, with a 12-hour light and dark cycle, at a temperature of 20°C with food and water ad libitum.
After 3 months, the animals were sedated with ethyl-ether, and the bone mineral density (g/cm 2 ) in the diaphysis region of the left femur was determined. A densitometer (Prodigy, GE Healthcare, Little Chalfont, United Kingdom), aided by the enCORE Software Platform (GE Healthcare, Little Chalfont, United Kingdom) adapted for small animals, was used.
The day after the densitometer examination, the animals in all 3 groups were anesthetized with an intramuscular injection of xylazine (0.1 mL/100 g) and ketamine (0.1 mL/100 g). The orthodontic appliances made up of a closed 7-mm nickel-titanium spring (Morelli, Sorocaba, São Paulo, Brazil) were placed. One millimeter of activation was performed to provide 40 cN. The appliance was anchored to the maxillary incisors and the maxillary left molar ( Fig 1 ), thereby producing a mesialization vector on the first molar. This procedure was carried out by using a restraint table.

The animals were killed 5 and 7 days after the placement of the appliance (n = 8 animals at a time per group). The maxillary right first molar of each animal was used as the control in all groups, since it did not receive orthodontic force. The rats were killed with an overdose of ketamine administered intraperitoneally. The maxillae were removed, dissected, and fixed in Bouin’s solution for 24 hours. The springs were removed and the pieces decalcified in 5% nitric acid for 4 days. The pieces were then embedded in paraffin, and the slices were cut 5 μm in thickness in the longitudinal direction and stained with hematoxylin and eosin.
Movement of the maxillary molar was determined by measuring the distance between the first and second molars from each cervical dental crown region (enamel edge) ( Fig 2 ). The measurements were made with a ruler coupled to an optical microscope (Olympus CBB, Tokyo, Japan) at a magnification of 10 times. The mean of the measurements was calculated on 10 histologic slices per animal for each group.
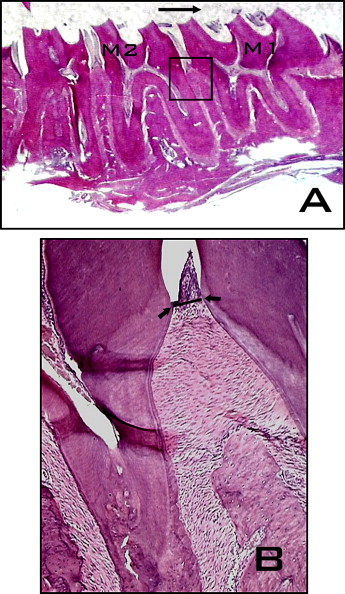
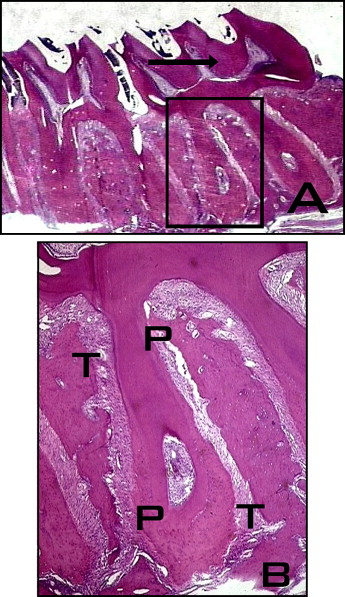
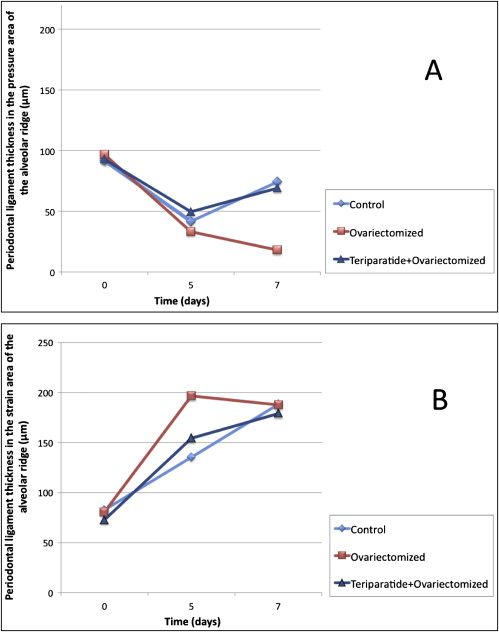
The thickness of the PDL was measured at the distal root apex and the alveolar ridge in the region of the root fork and in the areas of tension and pressure of the first molar’s PDL ( Fig 3 ). The same ruler coupled to an optical microscope (Olympus CBB) at magnification of 10 times was used. The measurements were made on 8 slices per animal. In each area of pressure or tension of each slice, the thickness of the PDL was the mean of the measurements taken at 3 points.
The number of osteoclasts was determined in the pressure area of the alveolar ridge of the first molar distal root. A 10 × 10 μm (Olympus) grid coupled to the eyepiece was used to delimit the count field. The counts were made on an optical microscope (Olympus CCB) at magnification of 20 times. The osteoclasts were quantified in 5 semiseries slices per animal, totaling 40 fields per area per group.
Statistical analysis
The Statistica software program (version 7.1, StatSoft, Tulsa, Okla) was used for the statistical analysis. Bone mineral density, rate of first molar movement, thickness of the PDL, and number of osteoclasts were analyzed by using 1-way analysis of variance (ANOVA). The Tukey post-hoc test was used for comparisons between means. The significance level was set at P <0.05.
Results
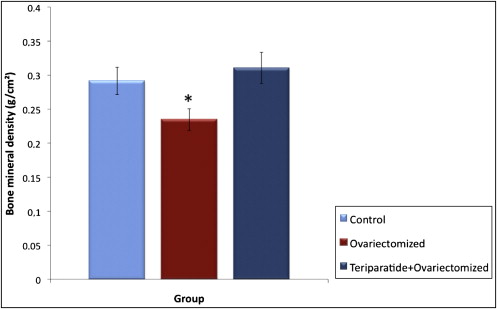
The densitometry evaluation (g/cm 2 ) showed an 11.2% reduction ( P <0.05) in bone mass (femur area) in the ovariectomized group (0.23 g/cm 2 ± 0.02) at 3 months after the surgery compared with the control group (0.29 g/cm 2 ± 0.02). There was complete restoration of bone density in the teriparatide and ovariectomized group (0.31 g/cm 2 ± 0.02) ( Fig 4 ).
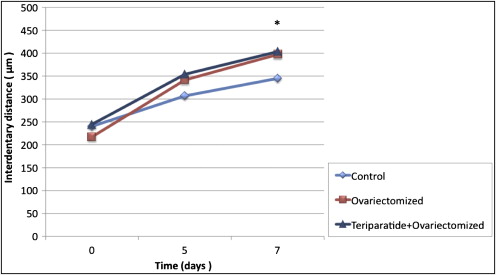
Significant molar movement ( P <0.05) occurred in all groups after 5 and 7 days. The ovariectomized groups with (403.5 μm ± 29.5) and without (397.3 μm ± 54.4) teriparatide exhibited greater movement ( P <0.05) rates after 7 days in comparison with the control group (345.0 μm ± 15.3) ( Fig 5 ).
There was an expressive variability in PDL thickness on the pressure and tension sides at the root-apex level in all groups. No significant differences were found.
Figure 6 , A , illustrates PDL thickness in the pressure area of the alveolar ridge region. There was a clear tendency toward a reduction in PDL thickness in all groups. A statistically significant difference was found between the initial thickness (96.6 μm ± 13.7), and that at 5 days (33.16 μm ± 32.0) and 7 days (18.02 μm ± 17.7) in the ovariectomized group.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


