Introduction
This study had 2 aims: (1) to assess whether the surgical exposure technique, the patient’s age, and the grade of impaction are associated with ankylosis of the impacted canine; and (2) to investigate the effect of rapid palatal expansion on an impacted canine’s automatic eruption.
Methods
The sample for this prospective longitudinal study consisted of 118 orthodontic patients (72 female, 46 male) who were treated surgically and orthodontically by the first author (S.I.K.) over 18 years. The patients’ ages at the beginning of therapy ranged from 11.2 to 46.1 years. They had 157 impacted canines (150 maxillary, 7 mandibular), grouped in 7 categories (grades I-VII) according to their radiographic position in the orthopantomogram at the onset of treatment. Univariate and multivariate generalized estimating equation logistic regression analyses were used to assess the effect of the predictors of interest on ankylosis. (In this research, a broad definition of “ankylosis” was used, to include impacted canines immobilized a priori or during traction, due to all the possible causes that could contribute to immobilization, such as all types of external tooth resorption and other known or unknown factors.)
Results
Thirty-eight canines erupted spontaneously after space gaining, and the other 119 were treated surgically with an open (57 cases) or a closed (62 cases) exposure technique. Eleven canines of the 119 that were treated surgically had ankylosis, either a priori or during orthodontic traction. The percentages of ankylosis were 3.5% in the open technique and 14.5% in the closed technique. Evidence of statistical association was found between age and ankylosis, grade of impaction and ankylosis, and rapid palatal expansion and automatic eruption of the impacted canine.
Conclusions
Evidence of an association between exposure technique and ankylosis was found. Additionally, there was evidence that the grade of impaction and the patient’s age are significant predictors of ankylosis, as is the use of rapid palatal expansion a predictor of automatic eruption.
There are numerous surgical procedures to expose an impacted canine and to bring it to its proper position in the dental arch. The open exposure technique allows natural eruption of the impacted canine; the closed exposure technique involves placement of an auxiliary attachment, which is then used for orthodontic traction. When the neighboring teeth are intruded and the canine remains immobile despite the application of orthodontic force, this is commonly recognized by clinicians as an indication of “ankylosis.”
The term ankylosis is generally associated with resorption (replacement root resorption). In ankylosis-related resorption, immobilization is observed clinically, since the root surface (cement or dentin) of the tooth is fused with the alveolar bone. In this study, we broadened the definition to include impacted canines immobilized a priori or during traction, due to the many possible causes that could contribute to immobilization, such as all the types of external tooth resorption and other known or unknown factors.
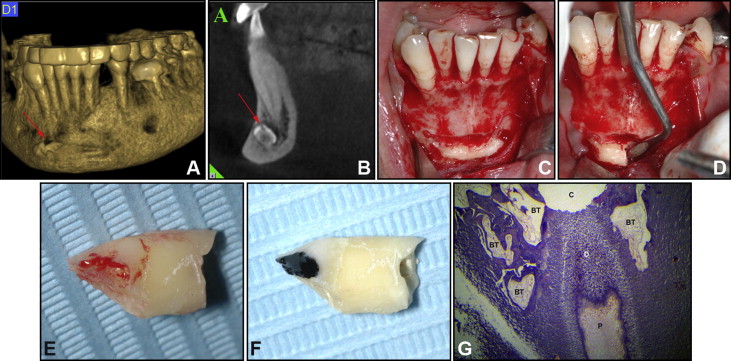
In the literature, the failure in the therapy of the impacted canine has been studied, but there are aspects of this failure that have yet to be considered. Indicatively, an unusual a priori ankylosis in the form of an ankylosis-related resorption of the crown (not the root) of the impacted canine is shown in Figure 1 . This process could lead to the failure of the therapy of the impacted canine.
Additionally, whether there is an association between surgical exposure technique, age of the patient, or severity of impaction and ankylosis has not yet been fully determined. Hence, the main objective of this study was to assess whether there is an association between ankylosis of the impacted canine and either the surgical exposure technique, the grade of its impaction, or the patient’s age. A secondary objective was to assess the effect of rapid palatal expansion on the automatic eruption of the impacted canine without surgical intervention.
Material and methods
All participants in this clinical study came from the private practice of the first author, who treated all the impacted canines surgically and orthodontically over a period of 18 years (1994-2012). No specific inclusion or exclusion criteria were applied, since all patients who agreed to undergo therapy were included.
The canines were considered impacted when their roots were fully developed but the teeth were still covered with bone or mucosa.
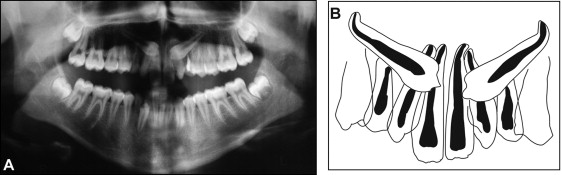
We implemented a new grading method to categorize the severity of canine impaction. The impacted canines were grouped into 7 categories, according to their radiographic position in the orthopantomogram at the onset of treatment. The position of the cusp tip and its relationship to concrete anatomic structures of the neighboring lateral and central incisors determined the grade of impaction (I-VII) as follows ( Figs 2 and 3 ).
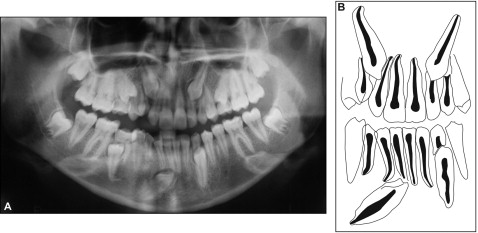
Grade I: The tip of the cusp has no contact with the distal aspect of the lateral incisor, regardless of the distance between the cusp tip and the plane of occlusion.
Grade II: The tip of the cusp touches, or can reach as far as, the distal aspect of the root canal of the lateral incisor.
Grade III: The tip of the cusp appears radiographically through the root canal of the lateral incisor and can reach as far as its mesial aspect.
Grades IV and V: The tip of the cusp can reach as far as the mesial aspect of the root canal of the central incisor; in grade V impaction, the tip of the cusp appears radiographically through the root canal of the central incisor and can reach as far as its mesial aspect or even the midline of the respective jaw.
For grades II to V, the tip of the cusp appears vertically on or below the border between the apical and coronal halves of the root of the lateral or central incisor in the maxilla, and on or above this border in the mandible.
Grade VI: The tip of the cusp is located above the border between the apical and coronal halves of the lateral or central incisors’ roots in the maxilla and below this border in the mandible.
Grade VII includes canines that are in transposition or transmigration in the maxilla or the mandible ( Fig 1 ).
The accurate location of the crown of the impacted canine was evaluated by examining the orthopantomogram and by clinical examination before the surgical exposure. This included intraoral palpation and meticulous observation of the characteristics of the anatomic structures (crown and root) of the adjacent teeth (premolars, deciduous canine, and incisors) and especially the lateral incisors.
Digital volume tomography (specifically, cone-beam computed tomography images) was used for diagnosis of the accurate position and verification of the ankylosis of the impacted tooth only in complicated cases ( Fig 1 ).
The following open surgical technique, with minimal modifications, was used. For palatally dislocated canines after local anesthesia, an incision was made as far as the cortical bone, following the palatal contour of the teeth in most patients from the mesial aspect of the central incisor up to the distal aspect of the first premolar. Then, a full-thickness mucoperiosteal flap was raised so that the exposed cortical plate allowed the surgeon, using a low-speed bur with careful cooling, to remove the bone that covered the canine’s crown approximately 1 to 2 mm above the cementoenamel junction as well as the follicular tissue from its socket. The cementoenamel junction area and other anatomic structures, such as the roots of the adjacent incisors, were respected. Consequently, the full-thickness flap was repositioned apically and sutured with 3-0 silk sutures. Finally, the tooth and the operative area were covered with a eugenol-free periodontal dressing (Coe-Pak; GC America, Alsip, Ill) for wound protection and short-term patient comfort. The dressing was positioned carefully, and we tried to place the dressing cover as apically as possible over the exposed crown, so that between the mucosa and the tooth crown there would be a layer of dressing. Under these circumstances, the proliferation of the gingival tissue was controlled, a quick covering of the tooth was prevented, and the tooth could erupt more freely without being impeded by the gingival tissue. The sutures were removed a week after the operation. After eruption, an auxiliary attachment was bonded onto the crown, and orthodontic traction was initiated.
The following closed surgical technique was performed. For palatally dislocated canines, the same surgical procedure as in the open surgical exposure technique was used under local anesthesia. For enamel surface preparation, 35% phosphoric acid in gel form was applied for 10 seconds, and an eyelet with a small metallic chain was bonded onto the tooth. This attachment (eruption appliance; GAC, Central Islip, NY) was the same for the whole period of the study. Finally, the full-thickness mucoperiosteal flap was placed in its original position and sutured with 3-0 silk sutures. One week after surgery, the sutures were removed, and the orthodontic traction began.
The rapid palatal expansion technique (banded rapid maxillary expander) was used extensively in our treatment to reduce premolar extraction therapy.
Statistical analysis
Demographic and clinical characteristics were investigated with descriptive statistics. Univariate and multivariate generalized estimating equation logistic regression with robust standard errors modeling was applied to assess whether surgical exposure technique, age (as a continuous variable), grade of impaction, sex, and location of the maxillary impaction (labial or palatal) were associated with ankylosis. For assessment of the effect of grade of impaction on the ankylosis, the grade VII category, which includes the most severe impaction in our categorization and the rarest cases, was excluded from the analysis, and the variable was dichotomized to the “nonsevere” group (grades I-V) or the “severe” group (grade VI). Additionally, the effect of rapid palatal expansion on the automatic eruption of the impacted canines was assessed. All analyses were implemented in the SPSS statistical package (version 15.0; SPSS, Chicago, Ill) and Stata (version 12.1; StataCorp, College Station, Tex).
Results
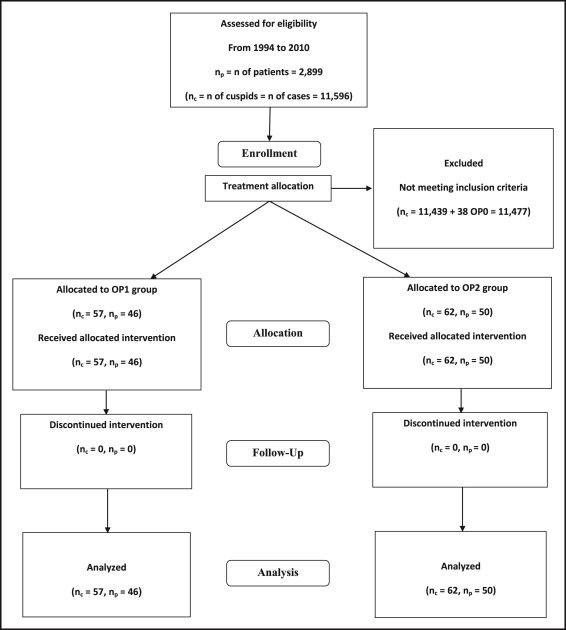
From 1994 to 2010, the number of patients who came to the surgery and remained for therapy after the diagnosis of a dental or skeletal problem of their maxillofacial system was 2899 (number of canines, 11,596). In 118 (4.1%) of these patients, the impaction of at least 1 canine was diagnosed.
This clinical study was based on 118 orthodontic patients, 72 female and 46 male, with 157 impacted canines. The CONSORT flowchart ( Fig 4 ) shows patient flow, and Table I gives the baseline characteristics of the study participants.
| Total (nc = 157) | OP0 (nc = 38) | OP1 (nc = 57) | OP2 (nc = 62) | |||||
|---|---|---|---|---|---|---|---|---|
| nc | Mean (SD) or % | nc | Mean (SD) or % | nc | Mean (SD) or % | nc | Mean (SD) or % | |
| Demographic characteristics | ||||||||
| Age (y) | ||||||||
| 11-17 | 112 | 14 (1.4) | 32 | 13.5 (1.2) | 38 | 14 (1.8) | 42 | 14.3 (1.5) |
| 18-46 | 45 | 28.4 (8) | 6 | 21.9 (4) | 19 | 26.1 (7.1) | 20 | 32.5 (7.6) |
| Sex | ||||||||
| Female | 96 | 61.1 | 21 | 55.3 | 31 | 54.4 | 44 | 71 |
| Male | 61 | 38.9 | 17 | 44.7 | 26 | 45.6 | 18 | 29 |
| Clinical characteristics | ||||||||
| Grade of impaction | ||||||||
| I | 13 | 8.9 | 9 | 23.7 | 1 | 1.8 | 3 | 4.8 |
| II | 37 | 23.6 | 20 | 52.6 | 10 | 17.5 | 7 | 11.3 |
| III | 31 | 19.7 | 8 | 21.1 | 13 | 22.8 | 10 | 16.1 |
| IV | 33 | 21 | 1 | 2.6 | 14 | 24.6 | 18 | 29 |
| V | 26 | 16.6 | – | – | 12 | 21.1 | 14 | 22.6 |
| VI | 14 | 8.9 | – | – | 6 | 10.5 | 8 | 12.9 |
| VII | 3 | 1.9 | – | – | 1 | 1.8 | 2 | 3.2 |
| Location of impaction | ||||||||
| Labial-maxilla | 36 | 22.9 | 24 | 63.2 | 4 | 7 | 8 | 12.9 |
| Palatal-maxilla | 114 | 72.6 | 12 | 31.6 | 52 | 91.2 | 50 | 80.6 |
| Labial-mandible | 6 | 3.8 | 2 | 5.3 | 1 | 1.8 | 3 | 4.8 |
| Lingual-mandible | 1 | 0.6 | – | – | – | – | 1 | 1.6 |
| Persistence of deciduous canine | ||||||||
| Yes | 112 | 71.3 | 18 | 47.4 | 47 | 82.5 | 47 | 75.8 |
| No | 45 | 28.7 | 20 | 52.6 | 10 | 17.5 | 15 | 24.2 |
From June 1994 to October 1996, the open surgical procedure was performed on all patients who came to the surgery. From November 1996 to May 2006, the closed surgical procedure was strictly used; for the latter period of the study (June 2006 to March 2010), the open surgical exposure was performed on all other patients who came to the surgery, except in 3 cases: 2 in the maxilla and 1 in the mandible.
The study sample included 150 impacted canines in the maxilla and 7 in the mandible. Thirty-eight canines erupted spontaneously after space gaining, and the other 119 were treated surgically by using open (57 cases) and closed (62 cases) exposure techniques.
The patients’ ages at the beginning of therapy ranged from 11.2 to 46.1 years (mean, 18.11 years; SD, 7.88). Eleven of the 119 surgically treated canines had the complication of ankylosis a priori or during their orthodontic traction.
The risk of ankylosis in the open exposure technique was 3.5% (2 of 57 canines); for the closed exposure technique, the risk was 14.5% (9 of 62 canines). In the younger age group (<18 years), 5.0% (4 of 77) showed ankylosis, whereas in the older group (>18 years), 17.9% (7 of 39) had ankylosis. In the “nonsevere” group (grades I-V), 6 cases (5.9%) showed ankylosis; in the “severe” group (grade VI), there were 5 cases (35.7%). The risks of ankylosis were 4.5% (2 of 44) and 12% (9 of 75) in male and female patients, respectively. Finally, the risk of ankylosis was 8.3% (1 of 12) in labially and 8.8% (9 of 102) in palatally impacted canines in the maxilla ( Table II ).
| Ankylosis nc (%) | No ankylosis nc (%) | |
|---|---|---|
| nc total = 11 (9.2) | nc total = 108 (90.8) | |
| Surgical exposure technique | ||
| OP1 (nc = 57) | 2 (3.5) | 55 (96.5) |
| OP2 (nc = 62) | 9 (14.5) | 53 (85.5) |
| Age | ||
| <18 (nc = 80) | 4 (5) | 76 (95) |
| ≥ 18 (nc = 39) | 7 (17.9) | 32 (82.1) |
| Grade of impaction | ||
| Nonsevere (I-V, nc = 102) | 6 (5.9) | 96 (94.1) |
| Severe (VI, nc = 14) | 5 (35.7) | 9 (64.3) |
| Sex | ||
| Male (nc = 44) | 2 (4.5) | 42 (95.5) |
| Female (nc = 75) | 9 (12) | 66 (88) |
| Location of impaction in the maxilla ∗ | ||
| Labial (nc = 12) | 1 (8.3) | 11 (91.7) |
| Palatal (nc = 102) | 9 (8.8) | 93 (91.2) |
Rapid palatal expansion was performed in 51 of the 150 maxillary cases. Twenty-three of those resulted in automatic eruption (45.1%), whereas, of the other 99 cases in the maxilla that did not receive rapid palatal expanison, only 13 (13.1%) resulted in automatic eruption (odds ratio [OR], 5.43; 95% confidence interval [CI], 2.43-12.14; P <0.001).
The results of the univariate and multivariate generalized estimating equation logistic regression with ankylosis as the dependent variable and surgical exposure technique (open or closed), age (continuous), severity of impaction (“nonsevere” group, grades I-V; “severe” group, grade VI), sex (male or female); and location of impaction in the maxilla (labial or palatal) as ankylosis predictors are shown in Table III . The automatic eruption cases (n = 38), the cases of grade VII (n = 3), and the impaction cases in the mandible (n = 7) were excluded from this analysis. The univariate analysis showed weak evidence of an association between ankylosis and surgical exposure technique and evidence of associations between age, grade of impaction, and ankylosis. No evidence of association between ankylosis and either sex or location of the impaction in the maxilla was detected. The multivariate analysis showed similar findings and reaffirmed that sex and location of impaction in the maxilla make no significant contribution to the prediction of ankylosis, whereas surgical exposure technique, age, and severity of impaction appear to be significant ankylosis predictors.
| Category | Univariable model | Multivariable model | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI for OR | P value | OR | 95% CI for OR | P value | |
| Surgical exposure technique | ||||||
| OP1 | Referent | Referent | ||||
| OP2 | 4.59 | 0.93-22.46 | 0.06 | 6.66 | 1.20-37.05 | 0.03 |
| Age | ||||||
| Referent | Referent | |||||
| Per unit | 1.01 | 1.04-1.02 | 0.001 | 1.11 | 1.03-1.19 | <0.01 |
| Grade of impaction | ||||||
| Nonsevere (I-V) | Referent | Referent | ||||
| Severe (VI) | 9.13 | 2.28-36.52 | 0.002 | 13.53 | 1.85-98.75 | 0.01 |
| Sex | ||||||
| Male | Referent | Referent | ||||
| Female | 2.89 | 0.60-14.10 | 0.30 | 2.10 | 0.53-7.99 | 0.30 |
| Location of impaction in the maxilla | ||||||
| Labial | Referent | Referent | ||||
| Palatal | 1.40 | 0.27-7.24 | 0.69 | 2.46 | 0.38-15.88 | 0.35 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


