Introduction
Our aim was to investigate the effect of rapid maxillary expansion and transpalatal arch therapy combined with deciduous canine extraction on the eruption rate of palatally displaced canines (PDCs) in patients in the late mixed dentition in a 2-center prospective study.
Methods
Seventy subjects were enrolled based on PDCs diagnosed on panoramic radiographs. The treatment group (TG, 40 subjects) underwent RME followed by TPA therapy and extraction of the deciduous canines. The control group (CG, 30 subjects) received no orthodontic treatment. At the start of the trial, panoramic radiographs and dental casts were compared between the TG and the CG with the Mann-Whitney U test ( P <0.05). At the second observation (cervical vertebral maturation stage 5 or 6), all subjects were reevaluated, and the eruption of the maxillary permanent canines was assessed. The rates of success in the TG were compared with those in the CG by means of chi-square tests ( P <0.05). The association of PDCs with other dental anomalies was reported.
Results
No statistically significant difference was found for any measurement at the start of the trial between the 2 groups. The prevalence rates of eruption of the maxillary canines were 80% for the TG and 28% in the CG, a statistically significant difference (chi-square =16.26, P <0.001). The prevalence rate at the start for the pubertal stages of cervical vertebral maturation (63%) was significantly greater in the unsuccessfully treated subjects than in the successfully treated ones (16%). In the CG, all successful subjects had PDCs that overlapped the corresponding deciduous canine or the distal aspect of the lateral incisor. Eruption of PDCs in both groups was associated significantly with an open root apex.
Conclusions
Rapid maxillary expansion therapy followed by a transpalatal arch combined with extraction of the deciduous canine is effective in treating patients in the late mixed dentition with PDCs. Pretreatment variables indicating success of treatment on the eruption of PDCs were less severe sectors of displacement, prepubertal stages of skeletal maturity, and open root apices of PDCs. Several dental anomalies were associated significantly with PDCs, thus confirming the genetic etiology of this eruption disturbance.
Palatal canine displacement (PCD) is a genetic disorder that is a precursor to palatal canine impaction, a dental anomaly that afflicts 0.2% to 2.3% of orthodontic populations. Treatment for palatal canine impaction involves surgical exposure and guiding mechanics to bring the canine into normal occlusion. Patients with PCD must be identified and treated promptly upon diagnosis to reduce the likelihood of impaction. Prevention of palatal impaction is of significant importance because canine impaction lengthens orthodontic treatment time, complicates orthodontic mechanics, and increases treatment costs. Furthermore, canine impaction can have deleterious consequences for adjacent teeth, causing root resorption or cyst formation.
The most common treatment for the prevention of palatal canine impaction is the extraction of the underlying deciduous canine. In a clinical trial, Ericson and Kurol reported an improvement in the eruption path of 78% of palatally displaced canines (PDCs) after extraction of the deciduous canine, and Power and Short reported a 62% successful eruption rate with the same interceptive technique. Another prospective longitudinal study conducted by Baccetti et al with an untreated control group indicated that 65% of patients with PDCs who had extraction of the deciduous canine resulted in successful eruption of the permanent canine with no other treatment. The prevalence rate of canine eruption can be improved significantly (up to 88%) by adding forces that prevent mesial migration of the maxillary posterior teeth after extraction of the deciduous canine, such as those exerted by cervical-pull headgear.
Recent data suggest that rapid maxillary expansion (RME) is a valid interceptive treatment option in patients with PDCs. A recent randomized clinical trial reported that RME therapy in the early mixed dentition prevented impaction in 66% of the PDC patients when compared with an untreated control group (14%). This study used posteroanterior radiographs to measure the distance of the palatally displaced canine cusp to the face midline to diagnose a PDC. Recent data have indicated that PDCs are not correlated to narrow maxillary arches. In this study, RME was performed on PCD patients with the primary aim of relieving mild-to-moderate crowding.
Our study was intended to evaluate further the impact of RME on the eruption rates of PDCs when interceptive treatment is carried out in the late mixed dentition; this has been indicated as an appropriate time to improve arch perimeter by maxillary expansion. The aim of this prospective controlled study was to assess the prevalence rates of successfully erupted PDCs diagnosed in the late mixed dentition by means of panoramic radiographs and subsequent treatment with RME, TPA, and deciduous canine extraction. Additional aims of this study were (1) to evaluate further the genetic origin of PCD by investigating its association with other dental anomalies of genetic origin and (2) to identify pretreatment variables associated with successful outcomes of interceptive treatment of PDCs with RME and TPA therapy.
Material and methods
The control and treated groups consisted of patients included in a 2-center prospective longitudinal clinical trial at the Department of Orthodontics and Pediatric Dentistry of the University Michigan and the Department of Orthodontics at the University of Florence in Italy. Criteria for enrollment of subjects in the clinical trial at the 2 research units were the following.
- 1.
White race.
- 2.
Age from 9.5 to 13.0 years at the start of treatment (T1).
- 3.
Late mixed dentition.
- 4.
Diagnosis of intraosseous malposition of at least 1 maxillary permanent canine, derived from the analysis of panoramic radiographs according to the method of Ericson and Kurol by means of alpha angle, d distance, and sector measurements. PDCs with an alpha angle ≥15° were included in the trial (milder forms of PCD were not included). PCD was confirmed by evaluating the position of the canine on the lateral cephalogram and, when necessary, with Clark’s tube shift rule by using multiple intraoral radiographs of the canine region. Such PDCs were either unilateral or bilateral.
- 5.
Stage of skeletal growth from cervical stage (CS) 1 to CS 4 as assessed on lateral cephalograms of the subjects according to the cervical vertebral maturation (CVM) method.
- 6.
Dentoskeletal Class II or Class III tendency or mild tooth size-arch length discrepancy.
- 7.
No previous orthodontic treatment.
- 8.
No supernumerary teeth, odontomas, cysts, craniofacial malformations, or sequelae of traumatic injuries.
A total of 70 subjects were enrolled at T1. They were allocated to 2 groups: treatment group (TG; 40 subjects, 25 girls and 15 boys) or control group (CG; 30 subjects, 18 girls and 12 boys). The TG subjects received treatment from 1 faculty group practitioner (J.A.M.) using a standardized treatment protocol, as described below. The CG subjects had no orthodontic treatment and were observed at the Department of Orthodontics of the University of Florence. Ethical approval was obtained for the enrollment of the subjects in the CG. Informed consent was signed by the parents of all subjects enrolled in the trial at both research sites.
Treatment protocol
The 40 subjects in the TG underwent RME. Thirty-five patients were treated with a bonded acrylic splint RME that covered the maxillary first and second deciduous molars and the maxillary first permanent molars, and the remaining 5 subjects, who had exfoliated deciduous molars, were treated with a banded RME with bands on the maxillary first permanent molars and first premolars. The midline expansion screw was expanded a quarter turn per day until expansion of about 7 mm was achieved (based on the number of turns recorded in the chart. The duration of active expansion was about 1.1 months, or approximately 5 weeks). After expansion, the RME appliance remained in place for an additional 4 to 5 months to allow for the reorganization of the disrupted sutural tissues. After removal of the RME, a TPA was placed on the maxillary first molars and activated according to the protocol described by McNamara and Brudon. Subjects who were not yet in the advanced late mixed dentition phase after expander removal wore a maxillary acrylic maintenance plate until TPA delivery when the maxillary second molars became loose. TPA treatment is postulated to prevent the mesial movement of the maxillary first molars during the transition to the permanent dentition. During TPA treatment, the retained maxillary deciduous canines corresponding to the PDCs were extracted. A primary goal for maxillary expansion in the TG was to improve the intraosseous position of PDCs. The CG received no orthodontic treatment.
Diagnostic measurements at T1
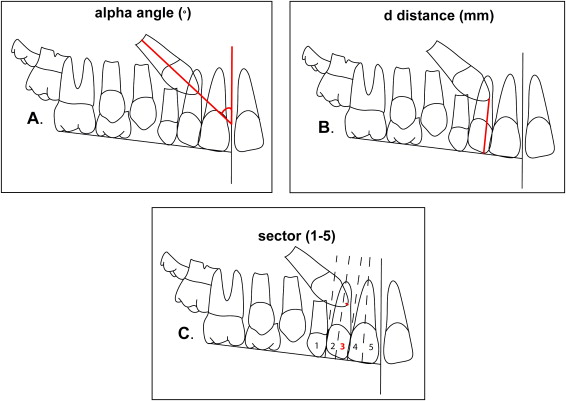
The panoramic radiographs of all subjects at T1 were analyzed. The following measurements proposed by Ericson and Kurol were made on the panoramic radiographs ( Fig ):
- 1.
Alpha angle: mesial inclination of the crown of the permanent canine to the midline ( Fig , A ).
- 2.
d distance: distance of the cusp tip of the permanent canine from the occlusal line ( Fig , B ).
- 3.
Sector: the mesial position of the crown of the displaced canine with respect to the central and lateral incisors (5 sectors, with sector 1 indicating the position of the crown of the displaced canine posterior to the distal aspect of the lateral incisor and sector 5 in correspondence with the mesial half of the maxillary central incisor) ( Fig , C ).
As indicated by Ericson and Kurol, these measurements are valid diagnostic variables for PDCs in the age range studied in this trial.
The CVM stage was evaluated on the lateral cephalograms of all subjects at T1. The development of the roots of all PDCs was appraised according to the method developed by Nolla.
The following measurements proposed by Tollaro et al were made on the dental casts at T1.
- 1.
Maxillary intermolar width: the distance between the central fossae of the maxillary right and left first molars.
- 2.
Mandibular intermolar width: the distance between the tips of the distal cusps of the mandibular right and left first molars.
- 3.
Posterior transverse discrepancy: the difference between the maxillary and mandibular intermolar widths.
In subjects with normal occlusion, the distobuccal cusp of the mandibular first molar occludes with the central fossa of the maxillary first molar. Consequently, in subjects with normal occlusion, maxillary and mandibular intermolar widths are equal. A negative posterior transverse discrepancy between the dental arches indicates a narrower maxillary measurement compared with the mandibular one.
Appraisal of dental anomalies associated with PCD
PDCs have been hypothesized to be part of a genetic cluster that includes other dental anomalies clinically associated with canine displacement. The TG and CG subjects analyzed in this study provided a sample of adequate size to investigate significant associations between PCD and the following dental anomalies : small maxillary lateral incisors, agenesis of second premolars, distally displaced erupting mandibular second premolars, and infraocclusion of deciduous molars. Small maxillary lateral incisors were defined as a severe crown-size reduction, in some cases associated with narrowing in diameter from the cervix to the incisal edge (peg-shaped lateral incisors). Distally displaced erupting mandibular second premolars were defined as an intraosseous anomalous position of the second premolar with its main axis cutting through the outline of the crown of the adjacent first permanent molar. Infraocclusion of deciduous molars occurs with ankylosis of the deciduous tooth, and the occlusal plane of the deciduous molar is apically positioned relative to the occlusal plane of the adjacent teeth.
The prevalence rates for these associations were contrasted with previously published control data from similar orthodontic populations of similar age ranges.
Reevaluation
According to the prospective design of the trial, all subjects were reevaluated at a second observation time (T2) when they were in the early permanent dentition with a postpubertal stage of CVM (CS 5 or 6). At T2, unerupted canines were considered impacted because the maxillary permanent canines will not erupt spontaneously after CS 5.
The number of dropouts was recorded. The main outcome investigated at T2 was successful or unsuccessful eruption of the maxillary permanent canines. A “successful outcome” for PCD was defined as the full eruption of the canine, thus permitting bracket positioning for final arch alignment when needed. An “unsuccessful outcome” was evident when there was no eruption of the permanent canine (impaction) at T2.
The magnification factor for the panoramic films in both groups was 18%. All measurements were performed with the primary investigator (L.M.S.) blinded to the groups.
Power of the study and method error
The estimate of the power of the study was performed before the clinical part of the trial. By considerating the standard deviations of the diagnostic measures on the panoramic radiographs from a previous study and by using nonparametric or categorical statistics, the calculated power of the study exceeded 0.90 at an alpha of 0.05 with the sample sizes of 40 and 30 subjects in the 2 groups.
The accuracy of the measurements on panoramic radiographs and dental casts was calculated with Dahlberg’s formula on measurements repeated on 15 subjects selected randomly from the 2 groups. The method errors were 1.3° for alpha angle, 0.7 mm for d distance, and <0.2 mm for the 2 dental cast measures. The appraisal of the sector of canine displacement showed reproducibility of 100%. Reproducibility for the assessment of dental anomalies associated with PCD was 100%.
Statistical analysis
The starting forms at T1 for measurements on panoramic films and dental casts were compared between the TG and the CG with the Mann-Whitney U test ( P <0.05). Maxillary and mandibular intermolar widths were contrasted with the same test to evaluate a possible interarch transverse discrepancy at T1. The rates of development of the roots of the displaced canines were compared in the 2 groups at T1 as well. The prevalence rates for sectors of canine displacement and for the stages in the CVM in the 2 groups at T1 were compared by means of the chi-square test ( P <0.05).
The prevalence rates for successful and unsuccessful subjects at T2 in the TG were compared with those in the CG with chi-square tests ( P <0.05).
The successful and unsuccessful groups as defined at the T2 reevaluation were compared with the following variables at T1: alpha angle, d distance, sector, age, CVM stage, and rate of bilateral PDCs. The rates of development of the root of displaced canines at T1 were compared in successful and unsuccessful subjects. These comparisons were carried out with Mann-Whitney U tests ( P <0.05) for metric measures and chi-square tests ( P <0.05) for categorical measures.
The TG and the CG were combined to calculate the prevalence rates for dental anomalies associated with PDCs. These rates were compared with those reported by Baccetti et al in 1998 and 2009 with chi-square tests ( P <0.05). The CG subjects in this study were derived from the same orthodontic population from which these prevalence rates were calculated. Statistical analysis was performed with software (version 16.0.1, Statistical Package for the Social Sciences, SPSS, Chicago, Ill).
Results
The number of dropouts from T1 to T2 was 1 subject in both the TG and the CG. These dropouts were due to the subjects’ relocating with their families during the observation period. The final samples ( Table I ) comprised 39 subjects (24 girls and 15 boys with 65 PDCs) in the TG and 29 subjects (17 girls and 12 boys with 48 PDCs) in the CG. The few dropouts did not affect the power of the study. The mean age at T1 for both groups was 10 years 5 months ± 10 months. The average age for the TG at T2 was 14 years 1 month ± 1 year 3 months, and the mean duration of observation was 3 years 7 months. The average age for the CG at T2 was 13 years 6 months ± 10 months, and the mean duration of observation was 3 years 1 month. There was no statistically significant difference in sex distribution between the TG and the CG.
| Age and age intervals | Treated group n = 39 | Control group n = 29 | TG vs CG | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mann-Whitney test | |
| Age T1 | 10 y 5 mo | 10 mo | 10 y 5 mo | 10 mo | NS |
| Age T2 | 14 y 1 mo | 1 y 3 mo | 13 y 6 mo | 10 mo | NS |
| Average T2-T1 interval | 3 y 7 mo | 1 y 5 mo | 3 y 1 mo | 1 y 2 mo | NS |
| Sex | Patients (n) | Percentage | Subjects (n) | Percentage | Chi-square test |
|---|---|---|---|---|---|
| Male | 15 | 38.5% | 12 | 41.4% | |
| Female | 24 | 61.5% | 17 | 58.6% | NS |
The descriptive statistics for the measurements on the dental casts and panoramic films at T1 in the 2 groups are reported in Tables II and III . The average maxillary intermolar widths were 43.3 ± 2.1 mm in the TG and 44.1 ± 2.1 mm in the CG; the average mandibular intermolar widths were 43.7 ± 1.9 mm in the TG and 44.3 ± 2.0 mm in the CG. Posterior transverse discrepancies were –0.7 ± 0.3 mm in the TG and –0.6 ± 0.3 mm in the CG. No statistically significant differences between the TG and CG were evident for any variable. The posterior transverse discrepancy in neither group was significant.
| Dental cast measurements | Treated group n = 39 | Control group n = 29 | TG vs CG | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mann-Whitney test | |
| Maxillary intermolar width (mm) | 43.3 | 2.1 | 44.1 | 2.1 | NS |
| Mandibular intermolar width (mm) | 43.7 | 1.9 | 44.3 | 2.0 | NS |
| Posterior transverse discrepancy (mm) | −0.7 | 0.2 | −0.6 | 0.3 | NS |
| Radiographic measurements | Treated group n = 39 |
Control group n = 29 |
TG vs CG | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mann-Whitney test | |
| Alpha angle (°) | 29.5 | 7.9 | 28.5 | 11.0 | |
| d distance (mm) | 16.9 | 2.8 | 17.5 | 3.9 | NS |
| Patients (n) | Percentage | Subjects (n) | Percentage | Chi-square test | |
|---|---|---|---|---|---|
| Sector 1 | 6 | 15.4% | 8 | 27.6% | NS |
| Sector 2 | 20 | 51.3% | 14 | 48.3% | |
| Sector 3 | 10 | 25.6% | 3 | 10.3% | |
| Sector 4 | 3 | 7.7% | 4 | 13.8% | |
| CS 1 | 14 | 35.9% | 7 | 24.1% | NS |
| CS 2 | 15 | 38.5% | 12 | 41.4% | |
| CS 3 | 8 | 20.5% | 10 | 34.5% | |
| CS 4 | 2 | 5.1% | 0 | 0.0% | |
| Unilateral | 12 | 30.8% | 10 | 34.5% | NS |
| Bilateral | 27 | 69.2% | 19 | 65.5% |
| Median | Range | Median | Range | Mann-Whitney test | |
|---|---|---|---|---|---|
| Root development of PCD | 8.75 | 7.25-9.50 | 9.00 | 7.50-9.75 | NS |
The comparison between the TG and the CG as to alpha angle, d distance, sector of canine displacement, CVM stage, and unilateral vs bilateral occurrence of PCD did not show any significant differences at T1. Root development of PDCs was similar in the 2 groups at T1 as well.
The prevalence rates for successful eruption of PDCs were 79.5% (31 subjects) in the TG and 27.6% (8 subjects) in the CG. The comparison was statistically significant (chi-square = 16.26; likelihood ratio = 19.05; P <0.001).
The comparison between successful vs unsuccessful subjects in the TG ( Table IV ) showed that, although there was no statistically significant difference for the alpha angle or the d distance, the prevalence rate for less severe sectors of canine displacement (sectors 1 and 2) was significantly greater in successfully treated subjects than in the unsuccessful ones. The prevalence rate at T1 for the pubertal stages of CVM (CS 3 or 4, 62.5%) was significantly greater in unsuccessfully treated subjectss than in successful ones, when 84% were in a prepubertal stage. In the CG ( Table V ), in all successful subjects, the PDCs were exclusively in sectors 1 and 2. The unsuccessful subjects in both groups had significantly more advanced development of the root of the displaced canine than did the successful cases. The percentage of subjects with root development stage 9 according to Nolla (closed root apex) was 4 times greater in unsuccessfully treated subjects than in successfully treated subjects ( Table IV ), and 2 times greater in unsuccessful control subjects than in successful control subjects ( Table V ). No differences were found regarding bilateral vs unilateral PCD with regard to canine eruption ( Tables IV and V ).


