Introduction
The primary stability of orthodontic anchorage miniscrews is believed to result from mechanical interlock, with success based upon a number of variables, including screw diameter, angle of placement, monocortical vs bicortical placement, placement through attached or unattached soft tissue, presence or absence of a pilot hole, periscrew inflammation, and maximum placement torque. The purpose of this ex-vivo study was to further explore the relationship between maximum placement torque during miniscrew placement and miniscrew resistance to movement under load.
Methods
Ninety-six titanium screws were placed into 24 hemi-maxillae and 24 hemi-mandibles from cadavers between the first and second premolars by using a digital torque screwdriver. All screws were subjected to a force parallel to the occlusal plane, pulling mesially until the miniscrews were displaced by 0.6 mm. The Spearman rank correlation test was used to evaluate whether there was an increasing or a decreasing relationship between maximum placement torque of the screws, miniscrew resistance to movement, and bone thickness. A paired-sample t test and the nonparametric Wilcoxon signed rank test were used to compare maximum placement torque, bone thickness, and miniscrew resistance to movement between coronally positioned and apically positioned screws in the maxilla and the mandible, and between screws placed in the maxilla vs screws placed in the mandible. Additionally, 1-way analysis of variance (ANOVA) with the post-hoc Tukey-Kramer test was used to determine whether there was a significant difference in miniscrew resistance to movement for screws placed with maximum torque of <5 Ncm, 5 to 10 Ncm, and >10 Ncm.
Results
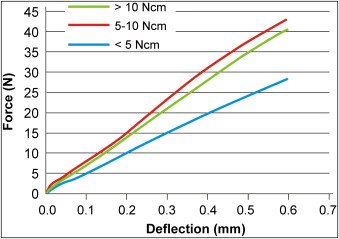
The mean difference in miniscrew resistance to movement between maximum placement torque groupings, <5 Ncm, 5 to 10 Ncm, and >10 Ncm, increased throughout the deflection range of 0.0 to 0.6 mm. As deflection increased to 0.12 to 0.33 mm, the mean resistance to movement for miniscrews with maximum placement torque of 5 to 10 Ncm was statistically greater than for screws with maximum placement torque <5 Ncm ( P <0.05). As deflection increased to 0.34 to 0.60 mm, the mean resistance to movement for miniscrews with maximum placement torque of 5 to 10 Ncm and >10 Ncm was significantly greater than for screws with maximum placement torque <5 Ncm ( P <0.05). At no deflection was there a significant difference in resistance to movement between the 2 miniscrew groups with higher placement torque values of 5 to 10 Ncm and >10 Ncm.
Conclusions
Ex vivo, the mean resistance to movement of miniscrews with higher maximum placement torque was greater than the resistance to movement of those with lower maximum placement torque.
The use of titanium miniscrews to provide orthodontic anchorage has become increasingly popular. In a 2008 survey of over 9000 orthodontists and orthodontic residents, it was found that 80% of the 564 respondents had at least 1 active patient involving miniscrews. Compared with traditional endosseous implants, miniscrews are smaller, easier and more versatile to place, and more cost-effective; they can be loaded immediately and are less painful postoperatively. The primary stability of miniscrews is believed to result from mechanical interlock with alveolar cortical bone. Since miniscrews do not achieve their primary stability through osseointegration, their anchorage potential is likely to be influenced by the quality and quantity of bone into which they are placed.
Screw placement torque has been suggested as a parameter in screw success or failure. A previous study reported that screws placed with a maximum placement torque in the range of 5 to 10 Ncm had significantly higher success rates compared with those placed with torque less than 5 Ncm or greater than 10 Ncm. However, this was a clinical study and leaves concern that variables other than placement torque played a role in the outcomes. The purpose of this ex-vivo study was to further explore the effect of maximum placement torque on a miniscrew’s resistance to movement under load.
Material and methods
The maxillae and mandibles of human cadavers were obtained from the Department of Anatomy and Cell Biology Deeded Body Program at the University of Iowa. Vital statistics of the cadavers were not available. Fully dentate and partially dentate specimens were considered acceptable. Fully edentulous or partially dentate specimens with visible, severely atrophic alveolar ridges were excluded. Maxillary specimens were dissected superior to the maxillary sinus to prevent damage to maxillary alveolar bones and tooth roots, with cuts extending distally to the maxillary tuberosity. Mandibular specimens were dissected approximately halfway up the ascending ramus. All maxillae and mandibles were subsequently hemi-sected, soft tissues were carefully removed, and the specimens were stored in 10% buffered formalin solution.
The site for placement of the screws was between the first and second premolars in both the maxilla and the mandible. Twenty-four hemi-maxillae and 24 hemi-mandibles were selected that met the inclusion criteria. If either the first or the second premolars were missing, the adjacent first or second premolar was used as a reference for its location based on average tooth size.
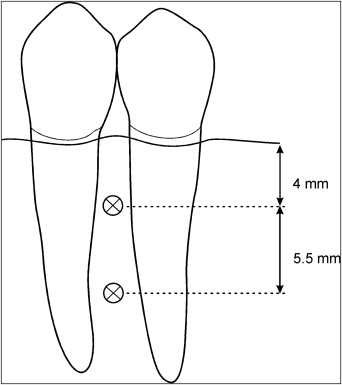
A total of 96 titanium screws (1.5 × 11 mm long; KLS Martin, Jacksonville, Fla) were placed in the 48 specimens. In each specimen, 2 screws were placed between the first and second premolars to a depth of 6 mm ( Fig 1 ), 1 coronally positioned and the other more apically positioned. The coronal screw was placed 4 mm apically to the maximal height of the interproximal crestal bone, and the apically positioned screw was placed 5.5 mm apically to the coronally positioned screw. The coronal distance was selected to ensure that all screws would have adequate bone and proper root divergence for placement without root contact. The apical distance was selected so that the screws would not be placed in the mental foramen or maxillary sinus areas, while maintaining adequate separation from the coronally positioned screw. Pilot holes were placed with the manufacturer’s recommended nontapered, 1.1-mm diameter twist drill (#25-452-15, KLS Martin).
All screws were placed by 1 operator (M.M.) with a manual digital torque screwdriver (model DID-4, Check-line Instruments by Electromatic, Cedarhurst, NY) with a customized milled insert ( Fig 2 ). The screws were placed at 90° to the bone surface. The digital torque screwdriver was set to measure maximum placement torque to the nearest 0.1 Newton-centimeter (Ncm). After verification of satisfactory screw placement, the most distal portion of each bony specimen was embedded in buff laboratory stone to a depth of 1.0 in and allowed to harden for 24 hours.

Each miniscrew was subjected to tangential force application oriented perpendicular to the placement of the miniscrew and parallel to the occlusal plane. This mimics the force placed on a miniscrew if it is used for retraction of anterior teeth. An Instron Diametral Materials Testing Machine (model 1445, Zwick, Ulm, Germany) was used; it incorporates a force transducer attached to a crosshead and is linked to a computer for recording the data. A customized x-y-z table with a mounting device was fabricated to rigidly fixate each stone block and cadaver specimen during testing. A customized grip was designed and machined from stainless steel to fit between the threads of each miniscrew. The custom grip was attached to the force transducer and oriented in a vertical position. The custom x-y-z table allowed for movement in 3 planes of space to ensure that the force was parallel to the occlusal plane. After orientation of the occlusal plane, the custom grip was attached to each miniscrew.
A crosshead speed of 0.05 mm per second was applied parallel to the occlusal plane. A similar crosshead speed was used in axial pullout studies of miniscrews. Displacement of the system was measured for approximately 1.5 mm, but only the first 0.6 mm of movement was investigated. This amount of displacement was selected to represent the amount of movement that would result in a clinically mobile miniscrew and potential failure.
Statistical analysis
After force application, each screw was removed, and the bone specimens were sectioned mesially and distally to the screw placement site with a diamond disk. Buccal plate alveolar bone widths were measured with a sharp, fine-tip digital calipers. Each measurement was made twice at screw placement sites, and the average of the 2 measurements was recorded. The Spearman rank correlation test was used to evaluate whether there was an increasing or a decreasing relationship between maximum placement torque of screws, miniscrew resistance to movement, and bone thickness. A paired-sample t test and the nonparametric Wilcoxon signed rank test were used to compare maximum placement torque, bone thickness, and miniscrew resistance to movement between coronally positioned and apically positioned screws in the maxilla and the mandible, or between screws placed in the maxilla vs screws placed in the mandible. Additionally, 1-way analysis of variance (ANOVA) with the post-hoc Tukey-Kramer test was used to determine whether there was a significant difference in miniscrew resistance to movement for screws placed with maximum insertion torque values of <5 Ncm, 5 to 10 Ncm, and >10 Ncm. The Tukey-Kramer test was used when sample sizes differed among groups. All tests had a 0.05 level of statistical significance. Statistical analyses were carried out with the SAS statistical package (version 9.1, SAS Institute, Cary, NC).
Results
A maximal placement torque of <5 Ncm was found for 42 miniscrews (11 mandibular and 31 maxillary sites), 5 to 10 Ncm for 40 miniscrews (23 mandibular and 16 maxillary sites), and >10 Ncm for 14 miniscrews (14 mandibular and 1 maxillary site). Mean miniscrew resistance to movement differences between these groupings was evident ( Fig 3 ) and increased throughout the deflection range of 0.0 to 0.6 mm. As deflection increased between 0.12 and 0.33 mm, mean resistance to movement for miniscrews with maximum placement torque of 5 to 10 Ncm was statistically greater than for screws with maximum placement torque <5 Ncm ( P <0.05). As deflection increased between 0.34 and 0.60 mm, mean resistance to movement values for miniscrews with maximum placement torque of 5 to 10 Ncm and >10 Ncm were significantly greater than for screws with maximum placement torque <5 Ncm ( P <0.05). At no deflection was a significant difference in resistance to movement found between the 2 miniscrew groups with higher placement torque values (5-10 and >10 Ncm).
A significantly increasing relationship between screw maximum placement torque and miniscrew resistance to movement was found at each deflection from 0.03 to 0.60 mm when all screws were considered together ( P <0.05 in each instance). The correlation coefficients from 0.20 to 0.51 indicated weak to moderate correlations between screw maximum placement torque and miniscrew resistance to movement. When maxillary screws were considered separately, a significantly increasing relationship between maximum placement torque and resistance to movement was found at each deflection from 0.01 to 0.60, with weak to moderate correlations (correlation coefficients, 0.33-0.69; P <0.05). When mandibular screws were considered separately, no statistically significant correlation was found between maximum placement torque and resistance to movement.
The thickness of the maxillary buccal cortical bone was 0.7 to 2.8 mm, with a mean of 1.62 ± 0.57 mm. The thickness of the mandibular buccal cortical bone was 1.02 to 4.18 mm, with a mean of 2.13 ± 0.66 mm. No significant relationship was found between bone thickness and miniscrew resistance to movement ( P >0.05) for all screws considered together, for maxillary screws alone, or for mandibular screws alone. A significantly increasing relationship was found between screw maximum placement torque and buccal cortical bone thickness when all screws were considered together with a moderate correlation (correlation coefficient, 0.53; P <0.00001). No significant correlation was found between maximum placement torque and buccal cortical bone thickness for maxillary screws, but a significantly increasing relationship was found between maximum placement torque and buccal cortical bone thickness for mandibular screws with a moderate correlation (correlation coefficient, 0.61; P <0.00001).
The mean maximum placement torque for screws in maxillary bone ( Table ) was 4.65 ± 3.37 Ncm (coefficient of variation, 72%); screws placed in mandibular bone had a mean maximum placement torque of 8.64 ± 5.42 Ncm (coefficient of variation, 62%). No significant difference was found in maximum placement torque, buccal bone cortical thickness, or resistance to movement between coronally positioned and apically positioned miniscrews in the maxilla or the mandible. Mean buccal cortical bone thickness and mean maximum screw placement torque were significantly greater in the mandible than in the maxilla ( P <0.001). Mean mandibular screw resistance to movement was significantly greater than in the maxilla for deflections from 0.20 to 0.60 mm ( P <0.05 in each instance).
| Quadrant | Screw number | Location | Torque (Ncm) |
|---|---|---|---|
| Mandibular right | 1 | Coronal | 7.9 |
| Mandibular right | 2 | Apical | 9.7 |
| Mandibular left | 3 | Coronal | 5 |
| Mandibular left | 4 | Apical | 5.3 |
| Mandibular right | 5 | Coronal | 5.8 |
| Mandibular right | 6 | Apical | 7.6 |
| Mandibular left | 7 | Coronal | 3.4 |
| Mandibular left | 8 | Apical | 2.8 |
| Maxillary right | 9 | Coronal | 5.8 |
| Maxillary right | 10 | Apical | 6.4 |
| Maxillary left | 11 | Coronal | 2.6 |
| Maxillary left | 12 | Apical | 0 ∗ |
| Maxillary right | 13 | Coronal | 2.5 |
| Maxillary right | 14 | Apical | 0 ∗ |
| Maxillary left | 15 | Coronal | 2.5 |
| Maxillary left | 16 | Apical | 3.7 |
| Maxillary right | 17 | Coronal | 3.6 |
| Maxillary right | 18 | Apical | 3.8 |
| Mandibular left | 19 | Coronal | 5.8 |
| Mandibular left | 20 | Apical | 3.5 |
| Mandibular right | 21 | Coronal | 4.6 |
| Mandibular right | 22 | Apical | 5.6 |
| Maxillary left | 23 | Coronal | 2 |
| Maxillary left | 24 | Apical | 4 |
| Maxillary right | 25 | Coronal | 3.6 |
| Maxillary right | 26 | Apical | 2.1 |
| Maxillary left | 27 | Coronal | 6.5 |
| Maxillary left | 28 | Apical | 6.9 |
| Mandibular right | 29 | Coronal | 7.3 |
| Mandibular right | 30 | Apical | 10.1 |
| Mandibular right | 31 | Coronal | 10.4 |
| Mandibular right | 32 | Apical | 11.9 |
| Maxillary right | 33 | Coronal | 2.5 |
| Maxillary right | 34 | Apical | 2.5 |
| Maxillary left | 35 | Coronal | 3.2 |
| Maxillary left | 36 | Apical | 2.7 |
| Maxillary left | 37 | Coronal | 9.7 |
| Maxillary left | 38 | Apical | 5.3 |
| Maxillary right | 39 | Coronal | 3.2 |
| Maxillary right | 40 | Apical | 4.1 |
| Maxillary left | 41 | Coronal | 2 |
| Maxillary left | 42 | Apical | 2.6 |
| Maxillary left | 43 | Coronal | 3.7 |
| Maxillary left | 44 | Apical | 5.8 |
| Maxillary left | 45 | Coronal | 5.7 |
| Maxillary left | 46 | Apical | 22.5 |
| Maxillary right | 47 | Coronal | 7.1 |
| Maxillary right | 48 | Apical | 5.6 |
| Maxillary right | 49 | Coronal | 3.5 |
| Maxillary right | 50 | Apical | 4.6 |
| Maxillary right | 51 | Coronal | 3.8 |
| Maxillary right | 52 | Apical | 3.6 |
| Mandibular right | 53 | Coronal | 10.6 |
| Mandibular right | 54 | Apical | 13 |
| Mandibular right | 55 | Coronal | 6.8 |
| Mandibular right | 56 | Apical | 2.7 |
| Mandibular left | 57 | Coronal | 4.5 |
| Mandibular left | 58 | Apical | 4.5 |
| Mandibular right | 59 | Coronal | 4.5 |
| Mandibular right | 60 | Apical | 4.2 |
| Mandibular left | 61 | Coronal | 9.5 |
| Mandibular left | 62 | Apical | 7.8 |
| Mandibular left | 63 | Coronal | 12.5 |
| Mandibular left | 64 | Apical | 6.7 |
| Mandibular left | 65 | Coronal | 24.2 |
| Mandibular left | 66 | Apical | 23.5 |
| Maxillary left | 67 | Coronal | 8.2 |
| Maxillary left | 68 | Apical | 9.2 |
| Mandibular left | 69 | Coronal | 9 |
| Mandibular left | 70 | Apical | 5.6 |
| Mandibular left | 71 | Coronal | 3.2 |
| Mandibular left | 72 | Apical | 3 |
| Mandibular left | 73 | Coronal | 8 |
| Mandibular left | 74 | Apical | 10.2 |
| Maxillary right | 75 | Coronal | 2.1 |
| Maxillary right | 76 | Apical | 2.7 |
| Maxillary right | 77 | Coronal | 4.7 |
| Maxillary right | 78 | Apical | 2.7 |
| Maxillary right | 79 | Coronal | 5.8 |
| Maxillary right | 80 | Apical | 5.7 |
| Mandibular right | 81 | Coronal | 6.4 |
| Mandibular right | 82 | Apical | 6.9 |
| Mandibular left | 83 | Coronal | 6.9 |
| Mandibular left | 84 | Apical | 7.3 |
| Mandibular right | 85 | Coronal | 21.7 |
| Mandibular right | 86 | Apical | 24.3 |
| Maxillary left | 87 | Coronal | 4.8 |
| Maxillary left | 88 | Apical | 4 |
| Mandibular right | 89 | Coronal | 7.2 |
| Mandibular right | 90 | Apical | 5.2 |
| Maxillary left | 91 | Coronal | 5.8 |
| Maxillary left | 92 | Apical | 7.6 |
| Mandibular left | 93 | Coronal | 12.2 |
| Mandibular left | 94 | Apical | 15.5 |
| Mandibular right | 95 | Coronal | 12.4 |
| Mandibular right | 96 | Apical | 8.2 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


