Introduction
Many researchers have examined the prevalence of dental injuries in children and adolescents. The purpose of this study was to examine the prevalence and incidence of incisor trauma in subjects who participated in a randomized clinical trial designed to investigate early growth modifications in the treatment of Class II malocclusion.
Methods
The subjects were randomized to 3 treatment groups during the initial phase of the study: (1) headgear or biteplane, (2) bionator, and (3) observation (no treatment). All 3 groups underwent phase 2 treatment with fixed appliances. Incisor injury was scored at every data collection point with the Ellis index by a blinded examiner using dental casts, intraoral photos, and panoramic and periapical x-rays.
Results
Twenty-five percent of the subjects had incisor trauma at the baseline examination, and 28% experienced new or worsening maxillary incisor injury during the study. No significant differences were found with regard to sex and prevalence of injury at baseline. No differences in incidence of trauma were found between the 3 treatment groups throughout the study ( P = 0.19); however, boys were more likely to experience maxillary incisor injury (odds ratio estimate, 2.37; 95% CI, 1.33, 4.21), and those with an injury at baseline were more likely to experience an additional injury (odds ratio estimate, 1.81; 95% CI, 1.03, 3.17).
Conclusions
Early orthodontic treatment did not affect the incidence of incisor injury. The majority of the injuries before and during treatment were minor; therefore, the cost-benefit ratio of orthodontic treatment primarily to prevent incisor trauma is unfavorable.
Dental injuries are common and are an important dental public health problem. Many epidemiologic studies during the last 3 decades have estimated the prevalence of dental injuries in children and adolescents. The occurrence of dental injuries in a population can be defined by its prevalence and incidence. The prevalence of incisor injury has been reported to range from 6% to 34%. Falls, collisions, sporting activities, and traffic accidents are the main causes of most dental injuries. Variables such as age, sex, socioeconomic status, and behavioral problems might also influence the frequency of dental trauma. Bauss et al and Caliskan and Turkun found that patients aged 8 to 11 years had the highest prevalence of dental trauma. It has been shown that incisor injuries occur more frequently in boys. Socioeconomic influences can also have a significant effect on a child’s experience with dental injuries. Studies have shown a positive correlation between the frequency of incisor trauma with increased protrusion, Class II malocclusion, increased overjet, and lip incompetence. Early orthodontic treatment for children with such characteristics has been recommended to prevent incisor trauma and its sequelae. Nguyen et al suggested the incorporation of overjet as a malocclusion item into orthodontic treatment indexes because of its potential correlation with dental trauma.
Although the indications for early orthodontic treatment to diminish the likelihood of trauma to permanent incisors have been presented by several authors, Koroluk et al found that most injuries were minor and easily treated at low cost and with good long-term prognoses. They concluded that early growth modification might have some effect on the incidence of trauma, with the expected cost of trauma per child to be less for those who had 2-phase orthodontic treatment.
The efficacy of early intervention largely depends on the timing of treatment and the peak occurrence of injuries. Orthodontic intervention could be ineffective with minimal benefits if dental trauma occurs before the start of treatment. Few reports are available regarding the effectiveness of early orthodontic treatment to reduce the incidence of incisor trauma.
The purpose of this study was to evaluate the prevalence and the effect on the incidence of incisor trauma in children who participated in a randomized clinical trial designed to investigate early growth modifications in the treatment of Class II malocclusion.
Material and methods
The subjects participated in a prospective, longitudinal, randomized clinical trial designed to examine the effectiveness of early treatment with headgear or biteplane or with bionator in children with Class II malocclusion and compare the results with changes over a similar time period in an observation group. The design, subject selection, and progression through the study were previously described in detail. The inclusion criteria included bilateral greater than or equal to one-half-cusp Class II molars or unilateral greater than one-half-cusp Class II molars, fully erupted permanent first molars, not more than 3 permanent canines or premolars, positive overjet and overbite, and good general and dental health. A stratified block randomization procedure was used to assign a treatment protocol (headgear or biteplane, bionator, and observation) during phase 1. Strata were defined by the severity of the Class II malocclusion (mild, bilateral half cusp; moderate, at least 1 side three quarters cusp; severe, at least 1 side full cusp), the need for preparatory treatment, mandibular plane angle, race, and sex. After completing phase 1, all groups underwent fixed appliance treatment in phase 2, followed by a retention or a follow-up period.
Incisor injury was assessed at all data collection (DC) points by using the modified Ellis classification ( Table I ). Maxillary and mandibular incisors were scored. Study models, intraoral and extraoral photos, x-rays (lateral cephalograms, panoramic radiographs, and periapicals taken during phase 2) obtained at each DC point were used to inspect incisor injuries. Any existing or new restorations on the teeth were noted. One trained and reliability-tested examiner (D.R.C.) recorded all injuries. The records for all DC points of each subject were evaluated at the same time to eliminate the chance of recording errors over time.
| Score | Injury description |
|---|---|
| 0 | Noninjured tooth |
| 1 | Fracture of the crown involving enamel only |
| 2 | Fracture of the crown involving enamel and dentin |
| 3 | Fracture of the crown involving pulp (untreated, pulp cap, pulpotomy, root filling) |
| 4 | Nonvital without crown fracture |
| 5 | Root fracture |
| 6 | Loss due to trauma |
| 7 | Missing tooth |
Overjet was assessed for each subject at all DC points by using the lateral cephalograms taken at each DC period.
Statistical analysis
Statistical comparisons considered intervals defined by the time points at baseline (DC 1), end of phase 1 active treatment (DC 3), end of phase 1 observation (DC 5), beginning of phase 2 (DC 7), and end of phase 2 (DC F). Relationships between outcomes and covariates were examined with the chi-square and Fisher exact tests. The Pearson correlation coefficient was used to examine the relationship between initial overjet and trauma. A generalized linear mixed model was used to examine the effect of multiple factors on new or increased injuries. Variables included in this model were incisor injury at baseline, treatment group, sex, time point, lagged overjet, and treatment group by time interaction. The lagged overjet variable used the previous time interval’s overjet measurement to examine the role of overjet at the start of a time interval on the occurrence of trauma during that time period. The treatment group by time interaction allowed for differences between treatment groups over time (eg, incidence could differ during the time interval of DC 1 to DC 3, with the observation group incurring more trauma, but then be similar for later time periods). As a secondary analysis, we examined the potential impact of a sex by treatment group interaction. For all analyses, a P value less than 0.05 was considered statistically significant.
Results
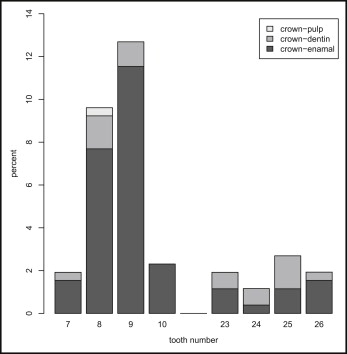
Table II presents the subjects’ characteristics by treatment group. At DC 1, 64 of the 261 participants (25%) had some incisor trauma (bionator, n = 27 [31%]; headgear or biteplane, n = 18 [19%]; observation, n = 19 [23%]). The differences in the proportion of subjects with trauma by treatment group were not statistically significant ( P = 0.18). Figure 1 shows the distribution and severity of injuries to maxillary and mandibular teeth. The majority (80%) of the injuries were scored as minor fractures involving enamel only. Fractures involving enamel and dentin accounted for 19%, and only 1 subject had trauma with pulpal exposure. The maxillary incisors had the most injuries (77%), with central incisors the most common. The prevalence of incisor trauma at DC 1 did not significantly differ between boys and girls ( P = 0.27), with 21% of the girls and 27% of the boys having some incisor trauma.
| Characteristic | Bionator (n = 87) | Headgear or biteplane (n = 93) | Observation (n = 81) | P value ∗ |
|---|---|---|---|---|
| Sex (% female) | 40 | 38 | 38 | 0.93 |
| Race (% white) | 87 | 95 | 93 | 0.20 |
| Initial molar classification | 0.95 | |||
| % Mild | 26 | 31 | 30 | |
| % Moderate | 26 | 23 | 26 | |
| % Severe | 47 | 46 | 44 | |
| Age (y) at DC 1, mean (SD) | 9.6 (1.1) | 9.7 (0.8) | 9.5 (0.8) | 0.72 |
| Overjet (mm) at DC 1, mean (SD) | 6.0 (2.8) | 5.4 (2.4) | 5.6 (2.6) | 0.41 |
∗ Chi-square tests used for categorical variables and analysis of variance (ANOVA) for continuous variables.
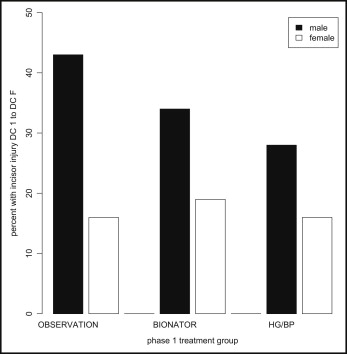
Since most injuries occurred in the maxilla, further analysis focused on the incidence of maxillary incisor injury. As shown in Table III , there were no differences in the incidence of new trauma between treatment groups during any time interval. As seen in Figure 2 , there was a significantly higher incidence of trauma in boys compared with girls during the entire study. During the study, only the observation group showed a significantly higher incidence of trauma in boys than in girls ( Fig 3 ).
| Time interval | Bionator | Headgear or biteplane | Observation | P value |
|---|---|---|---|---|
| DC 1-DC 3 | 13.8 (87) | 12.9 (93) | 13.6 (81) | 0.98 |
| DC 3-DC 5 | 11.7 (77) | 7.1 (85) | 12.5 (80) | 0.46 |
| DC 5-DC 7 | 4.3 (69) | 1.4 (74) | 6.7 (60) | 0.25 |
| DC 7-DC F | 3.2 (62) | 2.9 (68) | 10.9 (55) | 0.13 |
| DC 1-DC F | 28.4 (67) | 22.5 (71) | 33.3 (69) | 0.36 |

Overjet measurements were used to determine whether overjet correlated with trauma. The mean overjet values at baseline were 5.81 mm (SD, 2.77; range, 0.87-13.2) for boys and 5.48 mm (SD, 2.30; range, 0.51-11.2) for girls. No correlation was found between initial overjet value and the amount of maxillary incisor trauma at baseline (Pearson correlation coefficient, 0.02; P = 0.75). When evaluating baseline overjet and change in maxillary incisor injury as continuous variables throughout the study, a borderline significant correlation of 0.23 ( P = 0.0549) was found in the observation group, but not in the headgear or biteplane and the bionator groups (correlations, −0.11 and −0.06, respectively). The patterns of change in overjet for the 3 treatment groups are shown in Table IV .


