Introduction
Mandibular lateral displacement (MLD) is clinically characterized by deviation of the chin, facial asymmetry, dental midline discrepancy, crossbite in the posterior region, and high prevalence of internal derangement of the temporomandibular joint. Morphologic and functional characteristics of MLD should be clarified to correct and prevent this malocclusion.
Methods
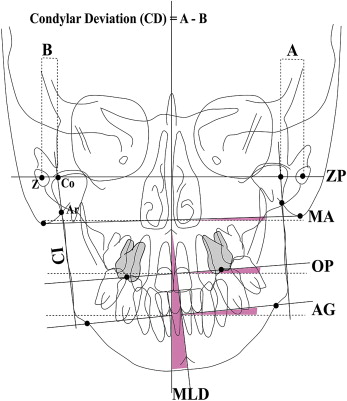
We examined the morphologic features, occlusal scheme, and functional behavior of MLD in 116 patients. Facial morphology was examined with posteroanterior cephalograms, occlusion guidance on the articulator after face-bow transfer, and condylar movement with the condylograph.
Results
The superiorly inclined occlusal plane was associated with mandibular deviation in the same direction. The posterior occlusal plane on the shifted side was significantly steeper than that on the nonshifted side. Functional analysis of condylar movement showed a close relationship between the direction of MLD and the direction of condylar lateral shift during opening and closing, and protrusion and retrusion. The occlusal guidance inclination in the buccal segment of the nonshifted side was steeper than that in the shifted side.
Conclusions
The results suggested that reduced vertical height of the dentition on 1 side induced mandibular lateral adaptation with contralateral condylar shift (asymmetry); this leads to condylar lateral shift during functional movement.
Editor’s comment
Although orthodontists realize the importance of correcting posterior crossbites in the mixed dentition or even earlier if possible, do we know why it is so critically important? What happens to the condyle, the developing dentition and adaptive alveolar bone, and even the cant of the posterior occlusal planes when this imbalance is not corrected? The authors of this study figured out how to retrospectively evaluate 116 patients with the morphologic features, occlusal schemes, and functional behaviors of MLD. Each patient’s MLD was examined with posteroanterior cephalograms and occlusal guidance on an articulator after face-bow transfer. Condylar movement was assessed with a condylograph. To completely understand the thoroughness of this investigation, read the entire description of this methodology online.
It was demonstrated that MLD is not due to simple mandibular lateral shift, but, rather, the mandible was 3-dimensionally rotated along with condylar displacement to the contralateral side. Therefore, it was speculated that decreasing or increasing the dental vertical height on 1 side because of several factors, such as postural habits, posterior discrepancy resulting in differences in eruption between the sides, or a difference in restorative heights between the sides leading to occlusal interferences, can be a risk factor for dysfuntional lateral shift of the mandible to the side of less vertical dimension. However, the etiology of skeletal asymmetry is multifactorial and a distinction can be drawn.
In concluding remarks, the authors noted, “Our results suggest that MLD is a problem that involves many factors such as occlusal vertical dimension, occlusal plane inclination, internal derangement of TMJs, functional ΔY shift of the condyle during function, occlusal guidance, and facial asymmetry.”