Introduction
The purpose of this study was to investigate the relative growth rates (RGR) of the maxilla and the mandible according to quantitative cervical vertebral maturation (QCVM) of adolescents with normal occlusion.
Methods
Mixed longitudinal data were used. The sample included 87 adolescents (32 boys, 55 girls) from 8 to 18 years of age with normal occlusion, selected from 901 candidates. Sequential lateral cephalograms and hand-wrist films were taken once a year for 6 consecutive years. The growth magnitude (GM) and RGR of the maxilla and the mandible were measured and analyzed.
Results
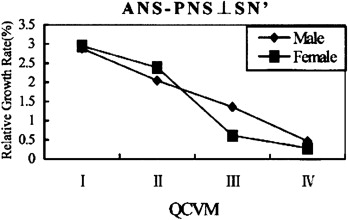
GM and RGR were not always consistent, because subjects had different periods of time between the QCVM stages. GM was not as reliable as RGR. RGR had no significant sex differences in the maxilla and the mandible, in spite of different decelerating curves. However, statistically significant sex differences were found in the GM of mandibular measurements. The greatest growth potentials were not synchronized between the maxilla and the mandible. For both sexes, the greatest RGR of maxillary length and height was in QCVM stage I; then, deceleration occurred. The greatest RGR of mandibular length and height was in QCVM stage II, and the next largest was in QCVM stage I.
Conclusions
Understanding the RGR can provide references for orthodontic treatment and orthognathic surgery.
Editor’s comment
During adolescence, growth rates accelerate until reaching a peak velocity, and then they decelerate until adulthood. Practitioners are aware of the marked individual variations in the start, duration, rate, and amount of this growth. Predicting craniofacial growth is a major concern to many orthodontists. To evaluate the rates of maxillary and mandibular growth in the different growth stages, a system of quantitative cervical vertebral maturation (QCVM) was proposed by Chen et al (Quantitative cervical vertebral maturation assessment in adolescents with normal occlusion: a mixed longitudinal study. Am J Orthod Dentofacial Orthop 2008;134:720.e1-7). Their methodology involves identifying specific maturational stages during the adolescent growth period. With that earlier work as a background, the purpose of this study was to provide an accurate index of acceleration and deceleration of the maxillary and mandibular growth rates, comparing them with the growth magnitude.
These researchers tracked growth of the maxilla and the mandible over a 6-year period, correlating the relative growth rates with the CVM indicators of Fishman (modified). Growth changes over varying periods of time were converted to annual rates. Interestingly, growth magnitude and relative growth rates were not always consistent. But of greatest interest to clinicians is the finding that the periods of greatest growth were not synchronized between the maxilla and the mandible. The greatest relative growth rate of maxillary length and height was in QCVM stage I, whereas, in the mandible, the greatest rate was in QCVM stage II. Therefore, the authors concluded that maxillary protraction to treat maxillary deficiency would be more effective when started at an early skeletal developmental phase or in QCVM stage I.
Despite the publication of new articles reporting the value of skeletal age assessment by CVM, the fact remains that vertebral shape is strongly correlated to skeletal age by assigning patients to broad categories instead of providing precise time estimates. Because this was a mixed longitudinal study that included the whole period of growth and development and looked retrospectively at growth with headfilms taken yearly, more information was gathered than would ever be possible with only 1 set of diagnostic records. Research findings are beginning to show that, without long-term records, predicting a patient’s peak growth rate from 1 headfilm is not much better than simply asking the patient’s age.