Introduction
In this study, we assessed the effects of age and sex on quality-of-life recovery after third-molar surgery.
Methods
Healthy subjects scheduled for removal of third molars were recruited at multiple sites for this study. Each patient was given a condition-specific instrument to be completed each postsurgery day for 14 days. Lifestyle and oral-function recovery were assessed by using a 5-point Likert-type scale. Recovery was defined as the number of days until the patient reported no or little trouble. Recovery from pain was defined as the number of days until no medications were taken. For each quality-of-life item, a Cox regression analysis was performed to assess the effects of age and sex on recovery after controlling for surgical-procedure variables.
Results
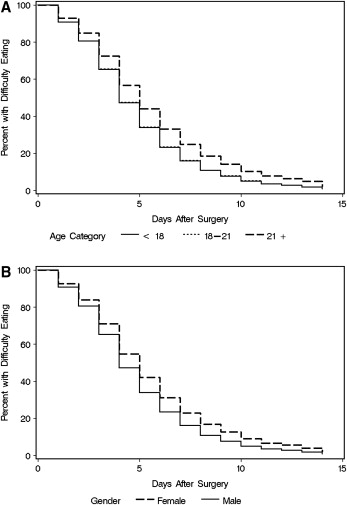
Nine hundred fifty-eight subjects treated at 9 academic centers and 12 community practices were enrolled. Except for ability to open the mouth, recovery for all quality-of-life items for those 21 years or older significantly ( P <0.02) lagged behind recovery for younger subjects. Recovery for female subjects was significantly longer than for male subjects for all outcomes ( P <0.01).
Conclusions
Patients older than 21 and those who are female should be informed before removal of all 4 third molars that their oral function, lifestyle, and pain recovery will be prolonged compared with those who are younger and male.
Editor’s comment
One problem I found difficult to discuss with any authority while in practice was the issue of third molars. Should they be extracted? And if so, when? Some surgeons recommend early extraction, before orthodontic treatment, and even before the third molar roots develop; others favor waiting until treatment is complete. Some clinicians, like me, prefer to be even more conservative and use the “wait and see” approach. But because active orthodontic treatment is often finished before the third molars erupt and jaw growth is complete, any recommendation for the third molars can be problematic. This study from the University of North Carolina was designed to assess the effects of age and sex on recovery of quality-of-life (QOL) outcomes, lifestyle, oral function, and pain after third-molar surgery in patients treated in either community practices or academic clinical centers.
QOL outcomes after third-molar surgery and surgical data were obtained from 958 subjects and their clinicians at 21 clinical centers (9 academic centers and 12 community practices). Participating surgeons in the community practices were fellows of the American Association of Oral and Maxillofacial Surgeons. The details of the study design are complete, and the discussion is quite interesting.
The results show that patients younger than 21 years of age, including adolescents completing orthodontic treatment, recover more quickly for QOL outcomes, pain, lifestyle, and oral function, compared with those 21 years and older. Age appears to be related not only to recovery after third-molar removal but also to clinical complications. The proportion of subjects who had an alveolar bone defect after surgery on the distal aspect of the second molars was significantly higher in the older cohort. These findings seem to make it even more critical for the clinician to make the extraction decision as early as possible. For me, this can still be a tough call.