Introduction
Treatment of impacted maxillary canines frequently requires surgical intervention, which can involve substantial complications. Thus, it is desirable to identify a reliable method for the early diagnosis of canine displacement. In this study, we sought to determine whether impaction of a maxillary canine can be predicted using measurements made on a panoramic radiograph.
Methods
This retrospective study was conducted at a dental hospital in Hong Kong with panoramic radiographs. Geometric measurements were made on 384 panoramic radiographs of patients with a unilaterally impacted maxillary canine (group I) to characterize its presentation and compare them with the unaffected antimere (group II).
Results
There was a clinically discernible difference of 4 mm at the age of 8 years and beyond between the mean distance of the tip of the impacted canine (group I) and that of the antimere (group II) from the occlusal plane ( P <0.05). Furthermore, there was a statistically significant difference at the age of 9 years and beyond between the 2 groups according to the position in different sectors and according to the mean angle made with the midline ( P <0.05).
Conclusions
Diagnosis of maxillary canine impaction is possible at 8 years of age by using geometric measurements on panoramic radiographs.
The fundamental aspect in the diagnosis of and treatment planning for an impacted maxillary permanent canine is the ability to recognize and predict its subsequent failure of eruption. Early diagnosis of canine displacement, in relation to the surrounding structures, is based primarily on a radiographic examination. Ericson and Kurol, who studied children aged 10 to 13 years, proposed that the diagnosis could be made using a panoramic film and that the time could be defined as “moderately” early. They used a series of geometric measurements made on panoramic radiographs that included the angle formed by the long axis of the canine with the midline, the vertical distance from the tip of the canine to the occlusal plane, and the distribution of the canine into different sectors depending on its location in relation to adjacent teeth. Furthermore, their final observations included the therapeutic effects of an interceptive approach such as extraction of a deciduous canine. Lindauer et al used a control group to develop a method to predict canine impaction at an accuracy of 78% with a modification of the procedure originally proposed by Ericson and Kurol. Overlapping of the lateral incisor by the canine on panoramic radiographs, when development of the incisor has been completed, can be considered a sign of a possible eruptive anomaly of the canine. Likewise, it has been shown that sector location is a significantly better predictor of impaction than tooth angulation. However, the relative diagnostic importance of these radiographic factors, including angulation of the canine to the midline, height from the occlusal plane, and buccopalatal position, has not been previously evaluated in Chinese children and adolescents.
Treatment of a palatally impacted canine usually involves surgical exposure and traction to move the tooth into the correct position. These procedures have high success rates but can involve substantial time and financial costs. They also carry risks of gingival recession, bone loss, and detachment of the gingiva around the treated canine. An interceptive treatment option includes extraction of the deciduous canine to prevent final impaction of the permanent successor. However, this method must first prove a positive diagnosis of canine displacement that will otherwise lead to canine impaction. Therefore, it is desirable to identify a method that can give the clinician a reliable protocol for early diagnosis of displacement of a canine and prediction of subsequent impaction.
A panoramic radiograph is a primary routine investigation for many patients. Hence, the variable, visible on that radiograph, could be used diagnostically to predict the impaction of a maxillary canine. This early diagnosis of an impaction can be used to determine the advantages, disadvantages, success rates, and clinical benefits of any operative technique. Thus, the objective of this study was to determine whether impaction of a maxillary canine can be predicted by using measurements made on a panoramic radiograph.
Material and methods
A total of 384 panoramic radiographs of 442 nonsyndromic patients known to have unilaterally impacted maxillary canines who had attended the Paediatric Dentistry and Orthodontics Clinic at Prince Philip Dental Hospital in Hong Kong SAR, China, were available for assessment. The clinical records and the radiologic data were used to assess and confirm the position of an impacted maxillary canine. The canine was defined as impacted if its antimere had completely erupted in the oral cavity, but the unerupted canine showed complete root formation radiographically ( Fig 1 ). The radiographs most commonly used to determine the position of the impacted canine are panoramic radiographs in combination with anterior occlusal films by using the vertical parallax principle and periapical radiographs taken at various horizontal angulations with the horizontal parallax technique. After the diagnosis had been confirmed from the clinical records and radiologic data, previous panoramic radiographs, if available, were traced to evaluate the position of the permanent canine of these patients. Thus, by using this mixed-longitudinal study design, the location of a canine was determined at different chronologic ages of a patient. All radiographs were examined in a darkened room by using an illuminated x-ray viewing box. The panoramic radiographs were traced with 0.003-in matte acetate tracing paper and a 0.5-mm HB fine lead pencil. Geometric measurements were made on the panoramic radiographs to show the impacted canine (group I) and to compare them with similar measurements made for the antimere tooth (group II). The measurements included the angulation and position (sector) of the tooth, the distance from the occlusal plane, and the stage of root development (adapted from Ericson and Kurol ).
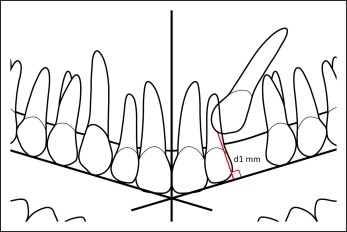
The occlusal plane was determined by drawing a horizontal line passing through the incisal edge of the central permanent incisor and the occlusal plane of the first permanent molar on the given side. When the central permanent incisor or the first permanent molar was absent, the lateral permanent incisor or the second permanent molar was used to determine the occlusal plane. In the deciduous dentition stage, the central incisor and the second molar were used to define the occlusal plane. A perpendicular line was then drawn from the incisal tip of the impacted canine and the antimere to the occlusal plane. This distance was called “d1” for the impacted canine group (group I) and “d0” for the antimere group (group II) ( Fig 1 ).
Groups I and II were categorized into different sectors depending on the location of the tip of the tooth in relation to the adjacent teeth ( Fig 2 ).

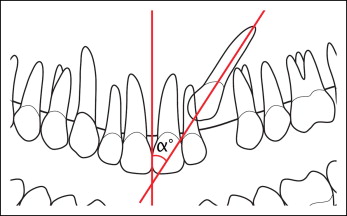
The angle formed by the long axis of the impacted maxillary canine (group I) with the midline was called “α,” and the angle formed by the long axis of the maxillary canine on the antimere side (group II) was called “” ( Fig 3 ). The midline was defined by the following landmarks on the radiograph: intermaxillary suture, anterior nasal spine, nasal septum, and internasal suture. When the tip of the canine was pointing in a direction opposite to the midline, a “−ve” sign was assigned as a prefix.
The root development of the canine was divided into 6 stages. The various stages and their interpretations were stage 0, root formation not yet begun; stage 1, root formation less than a quarter complete; stage 2, root formation between a quarter and a half complete; stage 3, root formation between a half and three quarters complete; stage 4, root formation more than three quarters complete; and stage 5, root formation complete.
All data were input into an Excel worksheet (version 2007; Microsoft, Redmond, Wash), and the data were printed out and checked for any keying-in errors. To determine whether there were any statistical differences between the geometric measurements made on the panoramic radiographs, the paired t test was used with the P value set at 0.05.
Results
The 384 panoramic radiographs that formed the sample for this study included parts of records from 111 patients with a total of 222 longitudinal follow-up radiographs. The data obtained from all 384 panoramic radiographs were divided into different age groups ( Table I ) to facilitate comparing the position of the impacted canine (group I) with the unaffected antimere (group II). This included 54 radiographs from patients in the age group of 3 to 8 years. No statistically significant difference was found between the values and measurements obtained for patients in whom the canines were buccally impacted and those in whom the canines were palatally impacted. Hence, the data were combined and the results further analyzed.
| Age of the patient (y) | Radiographs available (n) | Follow-up radiographs available (n) |
|---|---|---|
| 3 | 1 | 0 |
| 4 | 4 | 0 |
| 5 | 7 | 0 |
| 6 | 7 | 0 |
| 7 | 18 | 3 |
| 8 | 17 | 11 |
| 9 | 32 | 20 |
| 10 | 42 | 28 |
| 11 | 70 | 47 |
| 12 | 91 | 62 |
| 13 | 60 | 43 |
| 14 | 17 | 4 |
| 15 | 6 | 2 |
| 16 | 4 | 0 |
| 17 | 2 | 0 |
| 18 | 2 | 1 |
| 19 | 3 | 1 |
| 21 | 1 | 0 |
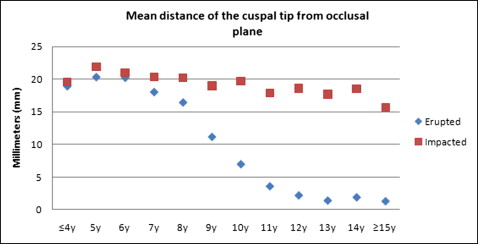
There was a statistically significant difference at the age of 5 years between the mean distance of the tip of the impacted canine (group I) and the unaffected antimere (group II) ( P = 0.01). All age groups beyond the age of 5 years also showed a highly statistically significant difference between the mean location of the impacted canine and the unaffected antimere ( Table II ). The mean distance covered by the impacted canine in the vertical direction from 5 to 12 years of age was 3.3 mm. During the same period, the mean distance covered by the unaffected antimere was 18.2 mm ( Fig 4 ).
| Age of patients (y) | Mean distance of impacted canine from occlusal plane (d1) | Mean distance of unaffected antimere from occlusal plane (d0) | Mean difference between groups (d1-d0) | P value |
|---|---|---|---|---|
| ≤4 | 19.6 | 19 | 0.6 | 0.3 |
| 5 | 21.9 | 20.4 | 1.4 | 0.01 ∗ |
| 6 | 21 | 20.3 | 0.7 | 0.04 ∗ |
| 7 | 20.4 | 18.1 | 2.3 | 0.04 ∗ |
| 8 | 20.2 | 16.5 | 3.7 | 0.001 ∗ |
| 9 | 19 | 11.2 | 7.8 | <0.0001 ∗ |
| 10 | 19.7 | 7 | 12.7 | <0.0001 ∗ |
| 11 | 17.9 | 3.6 | 14.3 | <0.0001 ∗ |
| 12 | 18.6 | 2.2 | 16.4 | <0.0001 ∗ |
| 13 | 17.7 | 1.4 | 16.3 | <0.0001 ∗ |
| 14 | 18.5 | 1.9 | 16.6 | <0.0001 ∗ |
| ≥15 | 15.7 | 1.3 | 14.4 | <0.0001 ∗ |
There was a statistically significant difference at the age of 9 years between the mean location of the impacted maxillary canine (group I) and the unaffected antimere (group II) according to the position in the sector ( P = 0.007) ( Table III ). All age groups beyond the age of 9 years showed a highly statistically significant difference between the mean location of the impacted canine and the unaffected antimere ( P <0.0001). The results demonstrated that, at the age of 9 years, the cusp tip of the impacted canine crosses the distal border of the lateral incisor to lie between the distal border and the midline of the lateral incisor ( Fig 5 ).
| Age of patients (y) | Mean sector location of impacted canine (S) | Mean sector location of unaffected antimere (N) | Mean difference between the groups (S-N) | P value |
|---|---|---|---|---|
| ≤4 | 0 | 0 | 0 | 1 |
| 5 | 0 | 0 | 0 | 1 |
| 6 | 0 | 0 | 0 | 1 |
| 7 | 0.3 | 0.2 | 0.1 | 0.5 |
| 8 | 0.6 | 0.3 | 0.3 | 0.3 |
| 9 | 1.0 | 0.2 | 0.7 | 0.007 ∗ |
| 10 | 1.2 | 0.1 | 1.1 | <0.0001 ∗ |
| 11 | 1.3 | 0.0 | 1.3 | <0.0001 ∗ |
| 12 | 1.7 | 0.0 | 1.7 | <0.0001 ∗ |
| 13 | 1.6 | 0 | 1.6 | <0.0001 ∗ |
| 14 | 2.3 | 0 | 2.3 | <0.0001 ∗ |
| ≥15 | 2 | 0 | 2.0 | <0.0001 ∗ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


