Introduction
Our aims were to evaluate long-term maxillary arch width changes in orthodontic patients treated with and without premolar extractions and to provide a potential link to the buccal-corridor ratios.
Methods
Dental casts of 34 extraction and 32 nonextraction orthodontic patients with Class I malocclusions were digitized and evaluated before treatment (T1), at posttreatment (T2), and at postretention (T3). The mean postretention times for the extraction and the nonextraction groups were 5 years 2 months and 4 years 10 months, respectively. Specific arch width measurements were made on the anatomic y-axis of the casts between the most labial aspects of the anatomic dental arch immediately distal to the incisive papilla, the farthest point posteriorly of the conjunction of the third lateral and medial rugae on the midpalatal raphe and at an individually constant distance from the incisive papilla. Arch width changes were calculated and compared statistically to determine whether the dental arches were narrower after extraction treatment and at postretention.
Results
All maxillary arch width measurements remained virtually stable after extraction therapy and at the postretention follow-up. Significant increases were recorded for all maxillary arch width measurements in the nonextraction group after treatment (mean changes, 1.37-2.05 mm). Posterior arch width measurements decreased significantly between T2 and T3 (mean change, 0.5 mm). Mean changes between T1 and T2 were significant between the 2 groups for all measurements ( P <0.05). Only the mean change in posterior arch width was significant between the 2 groups in the postretention period ( P <0.05).
Conclusions
Extraction treatment did not result in narrower maxillary dental arches, whereas nonextraction treatment slightly expanded the dental arch.
Among the transverse characteristics of the smile, arch form is considered of great importance to the clinician. Because narrow and collapsed arch forms can result in dark buccal corridors at the corners of the mouth during smiling, much attention has recently been paid to the use of broad, square arch forms. However, widening or changing the arch form remains controversial with respect to long-term stability.
On the premise that extraction of 4 premolars leads to narrowing of the dental arch width and decreased fullness of the dentition in the mouth during a smile, Johnson and Smith evaluated buccal-corridor ratios, the relationship of the width of the dentition to the soft tissue by ratios, on smile photographs after extraction and nonextraction treatments and concluded that there is no predictable relationship between the extraction of premolars and the esthetics of the smile. Because of claims that narrowing of the dental arches is the main cause of deterioration of buccal-corridor relationships, Gianelly compared anterior and posterior widths of the dental arches after both extraction and nonextraction therapies. His results indicated that maxillary arch widths measured between the canines and the second molars were the same after treatment. However, Spahl argued that posttreatment smiles should not be based on average values of specific width measurements, and posttreatment arch location should also be considered, since the posterior teeth would also move into the extraction spaces.
Because the premolar and molar anteroposterior positions might dramatically change after orthodontic treatment, another attempt was made by Kim and Gianelly to address the circumferential effects of tooth movement in the dental arches. In that study, arch widths were measured and compared at a constant arch depth representing the premolar-molar junction. Interestingly, arch widths of both groups measured from the most labial surfaces of the teeth at a constant depth differed significantly; they were wider in the extraction sample. Schack argued that retraction of canines in an extraction case would leave them in a wider part of the arch, increasing the intercanine width after treatment.
On the other hand, Kahl-Nieke et al stated that expansion is a significant factor in the process of postretention increase of crowding and incisor irregularity. However, an identical pattern of posttreatment relapse, which is related more to anteroposterior mandibular displacement than to the posttreatment dental relationships, was reported for extraction and nonextraction therapies. Furthermore, scientific articles have not differentiated between extraction and nonextraction patients in terms of changes in anterior irregularity over time.
Although the literature has provided some evidence that specific arch width measurement changes do not have a major effect on smile esthetics at the end of treatment compared with extraction and nonextraction treatment, those studies indicated many variables and conflicting points of view and yet lacked longitudinal evaluations. Our study was intended to address the long-term changes in maxillary arch width at 3 locations by using an individually standardized measurement technique after orthodontic therapy with and without extraction of 4 first premolars to report its potential impact, if any, on the smile.
Material and methods
The subjects were 66 patients from a graduate orthodontic clinic at the University of Oklahoma with Class I crowding who had treatment under the supervision of the same instructor (R.S.N.) using edgewise mechanics; all achieved acceptable posttreatment results. All patients had Class I canine and molar relationships and normal overjet and overbite with well-aligned and interdigitated teeth at the end of the treatment. Treatment records were obtained at 3 times: pretreatment (T1), posttreatment (T2), and postretention (T3). Retention was applied with Hawley retainers, and the postretention period was at least 3 years. The patients were divided into nonextraction (n = 32; 12 boys, 20 girls) and extraction (n = 34; 14 boys, 20 girls) groups. The mean ages at T1 were 14.2 ± 3.9 years for the extraction group and 13.8 ± 3.2 years for the nonextraction group. Pretreatment maxillary and mandibular incisor irregularity values as described by Little were 4.7 ± 3.2 mm and 5.8 ± 2.7 mm for the extraction group and 2.0 ± 2.1 mm and 2.3 and 2.2 mm for the nonextraction group, respectively. The treatment objectives were to ideally align the incisors, establish excellent occlusion with the teeth interdigitated, and resolve tooth size-arch length discrepancies while maintaining the original arch form. The retention period for both groups was between 30 and 38 months, with means of 34 ± 2 months in the extraction group and 33 ± 2 months in the nonextraction group. The mean treatment and the postretention times were 26 ± 3 months and 62 ± 4 months for the extraction group and 23 ± 3 months and 58 ± 3 months for the nonextraction group, respectively.
The inclusion criteria were (1) skeletal and dental Class I malocclusion, (2) normal growth pattern, (3) permanent dentition with no anomalies in crown morphology, (4) no occlusal wear and no dental restorations, and (5) no adjunctive appliances for lateral expansion.
Maxillary and mandibular canine, first premolar, and first molar widths were measured conventionally on the study casts with a digital caliper with a liquid crystal display output to define the arch widths at T1. A comparison of the arch widths at T1 in the extraction and nonextraction samples was done by independent-sample t tests to establish any arch width differences before treatment ( Table I ). No significant differences were found for any of these variables when comparing the 2 groups ( P >0.05).
| Variable | Extraction group | Nonextraction group | P | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Max 3-3 width (mm) | 36.04 | 2.21 | 36.27 | 2.18 | NS |
| Max 4-4 width (mm) | 39.17 | 2.55 | 40.13 | 2.17 | NS |
| Max 6-6 width (mm) | 51.81 | 3.02 | 52.01 | 2.98 | NS |
| Mand 3-3 width (mm) | 28.04 | 1.99 | 28.11 | 2.07 | NS |
| Mand 4-4 width (mm) | 33.90 | 3.08 | 34.60 | 2.95 | NS |
| Mand 6-6 width (mm) | 46.72 | 2.33 | 47.03 | 2.12 | NS |
Maxillary dental casts were digitized with a flatbed scanner (Epson EXP 1680 Pro, Seiko Epson, Nagano, Japan) with an 8-bit grey-scale acquisition depth and 400 dpi spatial resolutions. All digital images were saved in tagged image file format (TIFF) to a personal computer. The midincisal points of the incisors, the canine cusp tips, the buccal cusp tips of the premolars, and the mesiobuccal and distobuccal cusp tips of the first and second molars were used to establish the dental arch form on the images. The vertical axis (y-axis) was marked on the images by using 2 points: the point immediately distal to the incisive papilla and the farthest point posteriorly on the midpalatal raphe.
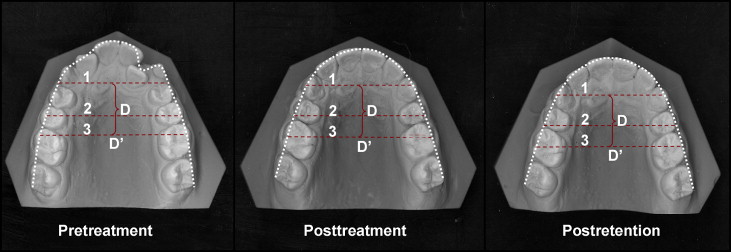
All measurements were made by computer with Image Tool for Windows (version 3.00, University of Texas Health Science Center, San Antonio, Tex). Spatial measurements were calibrated by drawing a line of known length (width of the maxillary central incisors). The following lines were drawn perpendicular to the y-axis of the images and measured in millimeters ( Fig ):
- 1.
Anterior width: between the most labial aspects of the anatomic dental arch immediately distal to the incisive papilla.
- 2.
Middle width: between the most labial aspects of the anatomic dental arch at the farthest point posteriorly of the conjunction of the third lateral and medial rugae on the midpalatal raphe.
- 3.
Posterior width: on the T1 images, between the mesiobuccal cusp tips of the maxillary first molars, with the distance from the point immediately distal to the incisive papilla to this line recorded as a constant individual distance (D) to further calculate the relative posterior arch widths on the T2 and T3 images; and, on the T2 and T3 images, between the most labial aspects of the anatomic dental arch at the relative individual D′ point.
All measurements were made by same investigator (B.D.), who repeated the measurements at 3-week intervals to ensure measurement accuracy using paired t tests. No differences were found in the remeasurements ( P >0.05). To determine the random error, 20 randomly selected cases from the whole sample were used. According to Dahlberg’s formula, SDe=√∑D2Nx2
S D e = ∑ D 2 N x 2
, where D is the difference between double determinations, posterior, middle, and anterior arch width measurements had error standard deviations ( SDe ) of 0.19, 0.28, and 0.18 mm, respectively. Error tests confirmed that the measurements were sufficiently reliable. The mean values of the first and second measurements for each parameter were used in later analysis.
Means and standard deviations were calculated for the T1, T2, and T3 measurements and the differences between the T1 and T2 measurements, and the T2 and T3 measurements. Kolmogorov-Smirnov normality tests were conducted for 3 parameters (anterior, middle, and posterior widths). Data for each measurement across the different time points in the extraction and nonextraction groups were normally distributed. Intragroup changes for T1 to T2 and T2 to T3 were evaluated with paired-samples t tests with the Bonferroni adjustment. A P value of 0.025 (0.05/2 = 0.025) was set as the significance level to control for type I error across the 2 pairwise comparisons (T1-T2, T2-T3). This correction was used for all measures (anterior, middle, and posterior widths). The independent-samples t test was used to compare the changes between the 2 groups for each time interval. All statistical analyses were performed by using the SPSS software package (version 13.0, SPSS for Windows, SPSS, Chicago, Ill).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


