Introduction
The aim of this study was to evaluate the significance of association between distally displaced premolars (DDP) and palatally displaced canines (PDC) in the pattern of associated phenotypes of dental developmental disturbance.
Methods
A sample of 2811 subjects (mean age, 9 years 7 months ± 1 year 3 months) was divided randomly into 2 groups. The first group of 500 subjects was the control group. The reference prevalence rates for the examined parameters were calculated for this group: DDP (measured with the distal angle and the premolar-molar angle γ); PDC; and other dental anomalies, specifically, aplasia of the third molars, aplasia of the contralateral mandibular second premolar, aplasia of the maxillary lateral incisors, and small maxillary lateral incisors. Of the remaining 2311 subjects, the first 100 with a diagnosis of DDP of at least 1 mandibular second premolar comprised experimental group 1 (DDP group). In addition to sex distribution, the same variables that were examined in the control group were analyzed. In the subgroup with the concurrent DDP and PDC (experimental group 2, or DDP-PDC group), the presence of other dental anomalies was investigated. The prevalence rate for PDC in experimental group 1 was compared with that in the control group. The same was done for the prevalence rates for the 4 other dental anomalies in the PDC-DDP group (experimental group 2) vs the prevalence rates for these anomalies in the control group. All comparisons were performed with chi-square tests with the Yates correction ( P <0.05), as were the comparisons between the sexes in experimental groups 1 and 2. The values for and γ angles in experimental group 1 were compared with the values for these angles in experimental group 2, as well as with those in the control group. These statistical comparisons were made with analysis of variance (ANOVA) with the Bonferroni post-hoc test ( P <0.05).
Results
The prevalence rate for PDC in experimental group 1 (28%) was significantly greater than in the control group (4.2%) ( P <0.01). Significantly greater prevalence rates for aplasia of the second premolars, aplasia of the maxillary lateral incisors, and small maxillary lateral incisors were found in the PDC-DDP group (experimental group 2) compared with the control group. Significant sex differences ( P <0.01) were found in both experimental groups.
Conclusions
A significant relationship between distal displacement of unerupted mandibular second premolars and PDC was found. Because DDP is diagnosed earlier than PDC, it can be a developmental risk indicator for displaced maxillary permanent canines.
During its development and eruption, the tooth germ of the mandibular second premolar is ideally positioned between the 2 roots of the deciduous second molar. Normally, the path of eruption follows a vertical direction through the resorption of the roots of the deciduous molar. However, abnormal tooth germ position and deviated angular changes during tooth eruption appear to be rather frequent, and they can lead to delayed eruption of the tooth until impaction. A specific feature is the distal inclination of the bud of the mandibular second premolar in relation to the adjacent first molar, a developmental tooth anomaly defined as distally displaced premolars (DDP). This condition is usually transitory and self-correcting when the second premolar erupts in the dental arch. Shalish et al demonstrated this anomalous distal inclination of the second premolar bud on the contralateral side in subjects with aplasia of the mandibular permanent premolars. They identified the association between the 2 dental disturbances as additional evidence of a shared genetic mechanism for dental anomaly patterns.
Similar considerations have been derived in the past from analysis of dental anomalies associated with palatally displaced canines (PDC). PDC is a dental anomaly with a genetic basis assessed in studies on the association between PDC and other tooth disturbances: aplasia of the mandibular premolars, aplasia of the maxillary lateral incisors, small maxillary lateral incisors, infraocclusion of the deciduous molars, and enamel hypoplasia. Interestingly, the clinical significance of these associations is that several of the dental anomalies potentially associated with PDC occur chronologically before the clinical recognition of the anomaly in the position of the maxillary permanent canine. Therefore, the clinician can use these associated dental anomalies for an early diagnosis of the likelihood of canine impaction.
The aim of this study was to evaluate the significance of the association between DDP and PDC in the pattern of associated phenotypes of dental developmental disturbances.
Material and methods
An initial sample of 3000 subjects in the early mixed dentition stage (before the exfoliation of the second deciduous molars) and at a cervical vertebrae maturation stage corresponding to CS1 or CS2 from the files of the Department of Orthodontics of the University of Florence in Italy was examined. All subjects were observed before any orthodontic treatment. Dental casts, intraoral photographs, and radiographic material (panoramic x-rays, lateral cephalograms) of all subjects were examined. Thirty-two subjects were excluded from the initial sample because of complex craniofacial malformations or cleft lip or palate (or both). Another 38 were excluded because they were siblings of other subjects, and 27 more because of bilateral aplasia of the mandibular second premolars shown by the panoramic x-ray. Another 92 subjects were excluded because of severe crowding in the mandibular arch, extensive caries (with special regard to the second deciduous molars), ectopic eruption of the mandibular first permanent molars, or impacted mandibular molars. The remaining sample of 2811 subjects (1348 boys, 1463 girls; mean age, 9 years 7 months ± 1 year 3 months) was divided randomly into 2 groups. The first group of 500 subjects included 231 boys and 269 girls (mean age, 9 years 8 months ± 1 year 1 month) and was the control group. The reference prevalence rates for the examined parameters were calculated for this group as follows.
- 1.
DDP was defined as the distal inclination of the bud of the mandibular second premolar toward the erupted permanent first molar. In each panoramic x-ray, the following structures were traced: the second deciduous molar, the bud of the mandibular second premolar, the neighboring mandibular first molar, and the lower border of the mandibular body near the second premolar and the first molar along with a line tangent to this lower border ( Fig 1 ). The long axis of the mandibular second premolar was determined as the line connecting the uppermost point of the pulp of this tooth with the point bisecting the distance between the mesial and distal points of the apex or the root canal. The long axis of the first molar was also traced. The stages of development of the unerupted mandibular second premolar had to range from stages E to G according to the classification of Koch et al : stage E is root length less than crown height, stage F is root length equal to or greater than crown height, and, in stage G, the walls of the root canal are parallel and the root apex is still partly open.
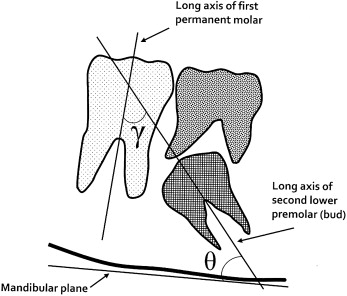
Fig 1 Angular measurements for the inclination of the mandibular second premolar bud on the panoramic radiograph.
DDP was measured with 2 angular measurements ( Fig 1 ): the distal angle (theta, ) is the angle between the long axis of the mandibular second premolar and the tangent to the lower border of the mandible on the panoramic x-ray (mandibular plane); the premolar-molar angle (gamma, γ) is the angle between the long axis of the mandibular second premolar and the long axis of the adjacent first permanent molar. The distal inclination of the mandibular second premolar was found to be an anomalous developmental intraosseous position of the tooth when the long axis of the premolar bud intersected the mesial border of the adjacent first permanent molar. When a subject had both unerupted mandibular second premolars with some distoangulation on the panoramic x-ray, the most distally displaced tooth bud was included in this study.
- 2.
PDC was defined according to the literature.
- 3.
Other dental anomalies were noted: specifically, aplasia of the third molars, aplasia of the contralateral mandibular second premolar, aplasia of the maxillary lateral incisors, and small maxillary lateral incisors. A small maxillary lateral incisor was defined as a severe crown-size reduction, sometimes associated with some narrowing in diameter from the cervix to the incisal edge (peg-shaped lateral incisors); a milder version of the latter form was also considered, with slight tapering of the crown from the gingiva to the incisal edge (“screwdriver-head” crown of the maxillary lateral incisor).
Of the remaining 2311 subjects (1096 boys, 1215 girls; mean age, 9 years 8 months ± 1 year 1 month), the first 100 with a diagnosis of DDP of at least 1 mandibular second premolar were selected: these subjects comprised experimental group 1 (DDP group). In addition to sex distribution, the same variables that were examined in the control group were analyzed: angulation of the DDPs and presence of PDC. In the subgroup with concurrent DDP and PDC (experimental group 2, or DDP-PDC group), the presence of the other abovementioned dental anomalies was investigated. The diagnoses of all dental anomalies, unilaterally or bilaterally, were made on dental casts and panoramic radiographs. Reproducibility of the diagnosis was assessed by reexamining the records of 100 subjects 1 month after the first examination by 1 operator (V.G.). Reproducibility was 100% for all dental anomalies except for small maxillary lateral incisors (94%). Method error for angular measurements was about 1.5° for both and γ angles.
Statistical analysis
The prevalence rate for PDC in experimental group 1 of 100 subjects with DDP was recorded and compared with the prevalence rate for PDC in the control group. The same was done for the prevalence rates for the 4 other dental anomalies in the PDC-DDP group (experimental group 2) vs the prevalence rates for these anomalies in the control group. All comparisons were performed with chi-square tests with the Yates correction ( P <0.05), as well as the comparisons between the sexes in experimental groups 1 and 2.
The values for and γ angles in experimental group 1 of 100 subjects with DDP were compared with the values for these angles in the group with concurrent DDP and PDC (experimental group 2), as well as with those in the control group. These statistical comparisons were performed with analysis of variance (ANOVA) with Bonferroni post-hoc tests ( P <0.05).
Results
Descriptive statistics and the results of statistical analyses are reported in Tables I and II .
| DDP group (experimental group 1) n = 100 |
DDP + PDC group (experimental group 2) n = 28 |
Control group n = 500 |
ANOVA with post-hoc tests (significance) |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Mean | SD | Mean | SD | Mean | SD | DDP vs control |
DDP + PDC vs control |
DDP vs DDP + PDC |
| γ angle (°) | 38.1 | 4.6 | 39.0 | 4.4 | 7.1 | 6.2 | ∗ | ∗ | NS |
| angle (°) | 56.7 | 3.4 | 58.2 | 4.2 | 85.4 | 4.7 | ∗ | ∗ | NS |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


