This case report describes the orthodontic treatment of an 18-year-old woman with a skeletal Class III malocclusion and a midline deviation. The treatment plan consisted of distalizing the mandibular dentition asymmetrically and producing space for retraction of the mandibular anterior teeth. Short Class III elastics, an open-coil spring, and the mulitloop edgewise archwire technique were used, combining the entire maxillary dentition as integrated anchorage. The active treatment period was 26 months. Normal overbite and overjet were obtained, and facial balance was improved.
A skeletal Class III malocclusion is a common orthodontic problem, with a prevalence of 8% to 22% of all orthodontic patients. For an adult patient with no potential for growth, treatment approaches depend on the growth, severity of the skeletal discrepancy, facial profile, and the patient’s desires. Generally, this malocclusion can be corrected by camouflage orthodontic treatment or orthodontic treatment combined with orthognathic surgery. In some borderline cases, the patient’s opinion of the soft-tissue profile plays a decisive role in treatment planning. For patients with an acceptable facial profile, camouflage treatment is the best choice, and various methods have been used, including multibrackets with Class III elastics with or without tooth extractions. Class III elastics often result in unexpected rotation of the mandible and proclination of the maxillary incisors and extrusion of the molars. This can cause an esthetic problem and instability, especially in long-faced adults.
Therefore, microscrew and miniplate implant anchorage for distalization of the mandibular posterior teeth was introduced. However, some patients do not readily accept this invasive approach because of the high cost and the risk of various complications, including injury to adjacent structures, inflammation, infection around the implant site, failure, and fracture. The goal of providing these patients a satisfactory facial profile and a stable occlusion without microimplant anchorage is worth consideration.
The purpose of this case report is to present an adult with a skeletal Class III malocclusion and a midline deviation treated with fixed orthodontic appliances, short intermaxillary elastics, and an open-coil spring to move the mandibular molars distally. This treatment produced a satisfactory facial profile and a stable occlusion.
Diagnosis and etiology
An 18-year-old woman was referred to Department of Orthodontics, West China School of Stomatology, Chengdu, China, for treatment, with the chief complaint of dissatisfaction with her dental alignment. Cephalometric and panoramic radiographs, extraoral and intraoral photographs, and dental casts were obtained.
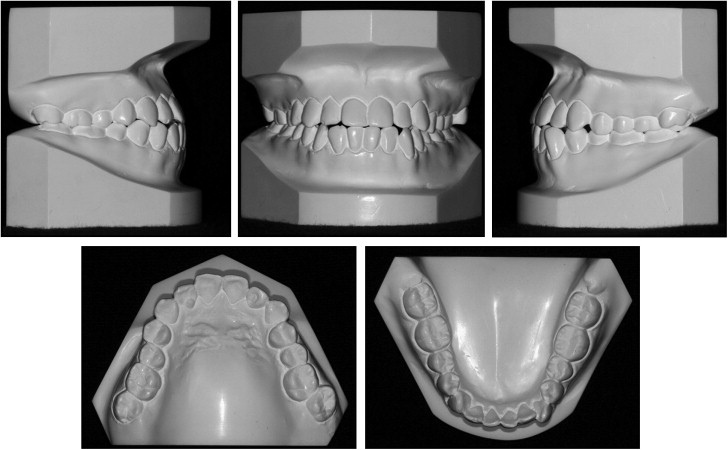
The extraoral examination ( Fig 1 ) showed that she had a relative long lower face and an acceptable profile with a slightly protrusive chin. The intraoral examination ( Fig 1 ) showed a complete Class III molar relationship on the left and a mild Class III malocclusion on the right, and Class III canine relationships bilaterally. There was an edge-to-edge anterior occlusion, and the maxillary left second molar was positioned buccally and overerupted. Mild crowding of 2.5 mm was present in the mandibular anterior region, and a little crowding was found in the maxillary dentition. The maxillary midline was coincident with the facial midline, whereas the mandibular midline was deviated 2 mm to the right side ( Fig 2 ). The functional examination showed no abnormal features, and there were no symptoms of temporomandibular disorder. The patient was in good general health with no history of major systemic diseases.
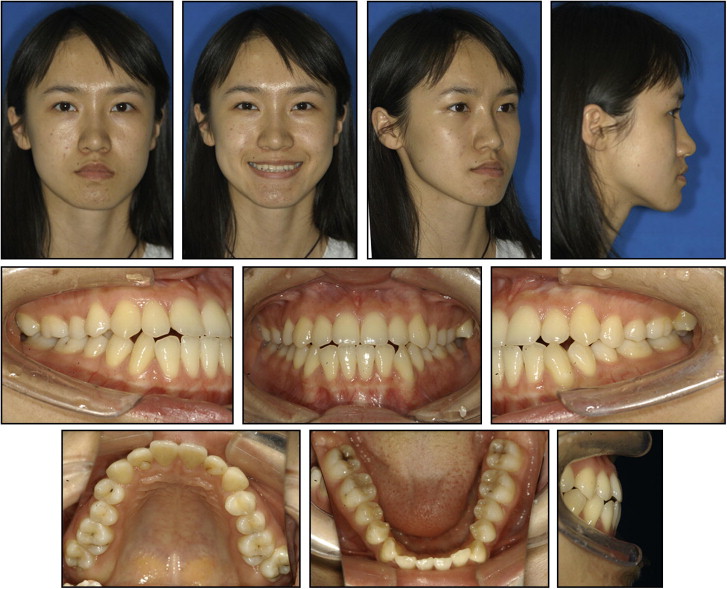
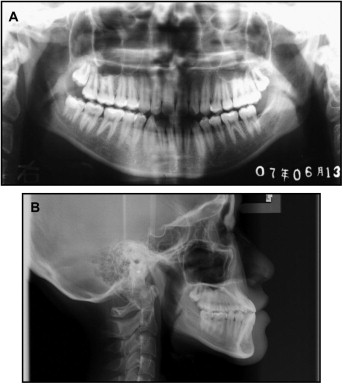
The lateral cephalometric analysis ( Fig 3 ; Table ) indicated a skeletal Class III jaw relationship (ANB, –3.4°) with mandibular protrusion (SNB, 85.2°). The mandibular plane angle (MP-SN, 36.0°) had a mild vertical growth pattern. The maxillary incisors were labially proclined (U1-NA, 32.0°), and a lingual inclination was observed at the mandibular anterior teeth (IMPA, 86.8°). The panoramic radiograph showed that all teeth were present except for the mandibular left third molar, and the maxillary and mandibular right third molars were impacted.
| Measurement | Normal mean | SD | Pretreatment | Posttreatment |
|---|---|---|---|---|
| SNA (°) | 81.69 | 2.54 | 81.8 | 83.2 |
| SNB (°) | 78.94 | 2.19 | 85.2 | 84.1 |
| ANB (°) | 2.75 | 1.16 | −3.4 | −0.9 |
| MP-SN (°) | 32.85 | 4.21 | 36.0 | 37.6 |
| UI-LI (°) | 123.22 | 6.18 | 132.4 | 120.8 |
| U1 to NA (mm) | 5.56 | 3.6 | 9.9 | 9.1 |
| U1 to NA (°) | 23.26 | 6.17 | 32.0 | 36.4 |
| L1 to NB (mm) | 5.76 | 2.29 | 5.0 | 5.5 |
| L1 to NB (°) | 27.38 | 4.74 | 28.0 | 23.7 |
| FMIA (°) | 54.6 | 6.5 | 64.8 | 68.5 |
| IMPA (°) | 96.3 | 5.8 | 86.8 | 82.0 |
| UL-EP (mm) | −0.46 | 1.92 | −2.6 | −1.2 |
| LL-EP (mm) | 1.31 | 1.92 | 0.1 | 0.7 |
The patient was diagnosed with a dental Class III malocclusion, a mandibular midline deviation, mandibular incisor crowding, and a skeletal Class III jaw relationship caused by the mandibular protrusion.
Treatment objectives
The treatment objectives were to (1) correct the anterior edge-to-edge occlusion and establish a normal incisor relationship, (2) achieve Class I molar and canine relationships by uprighting and distalizing the mandibular posterior teeth, (3) resolve the crowding in the mandibular arch, (4) correct the mandibular midline deviation, and (5) maintain the straight pretreatment facial profile.
Treatment objectives
The treatment objectives were to (1) correct the anterior edge-to-edge occlusion and establish a normal incisor relationship, (2) achieve Class I molar and canine relationships by uprighting and distalizing the mandibular posterior teeth, (3) resolve the crowding in the mandibular arch, (4) correct the mandibular midline deviation, and (5) maintain the straight pretreatment facial profile.
Treatment alternatives
Three treatment options were considered and presented to the patient. The first alternative consisted of combined surgical and orthodontic treatment with a mandibular setback. This proposal would be the best way to modify the skeletal pattern and produce a dramatic facial profile change. The second consisted of camouflage orthodontic treatment with extraction of the mandibular left first premolar. This would be a relatively simple and stable way to resolve the anterior crossbite, but there would be no contact between the maxillary left second molar and the opposing tooth. The other treatment alternative was a nonextraction camouflage orthodontic approach with distalization of the mandibular dentition. If the mandibular left second molar could not be distalized effectively because of the maxillary left second molar, the latter tooth would be extracted and replaced by the third molar. This would solve the problems of the posterior malposition and the molar relationship at the same time.
The patient refused the orthodontic-surgical treatment because she did not think that the esthetic improvement with surgery would be worth the risk and cost. She chose the third plan of distalizing the mandibular dentition because she cared about her dental and facial midlines and wanted to obtain complete function of her posterior teeth.
In most skeletal Class III cases, intraoral or extraoral anchorage is required to retract the mandibular dental arch. There were 2 anchorage alternatives for this patient to choose from. One was distalizing the mandibular posterior dentition with a microimplant combined with intra-arch elastics. The other was interarch elastics with the whole maxillary dentition as anchorage to retract the mandibular arch, with an open-coil spring to move the mandibular left molars distally. The patient was concerned about the invasive approach with potential complications and additional costs and refused the placement of a microimplant.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


