Introduction
Our objective was to investigate the dimensional accuracy of digital dental models obtained from the cone-beam computed tomography (CBCT) scans of alginate impressions according to the time elapsed after the impressions were taken.
Methods
Alginate impressions were obtained of 20 adults using 2 alginate materials: Alginoplast (Heraeus Kulzer, Hanau, Germany) and Cavex (Cavex Holland, Haarlem, The Netherlands). These impressions were stored in wet conditions and scanned by CBCT immediately after impression-taking and after storage times of 12, 24, 36, 48, 60, and 72 hours. After reconstruction of the 3-dimensional digital dental models, the models were measured, and the data were analyzed to determine the dimensional changes according to the time elapsed. The changes within the measurement error were regarded as clinically acceptable in this study.
Results
The measurement errors ranged from 0.27 to 0.29 mm in the digital dental models obtained from CBCT scans of the alginate impressions. All measurements showed decreasing accuracy with greater elapsed time after the impressions were taken. Changes above the measurement error occurred at 24 and 36 hours for Cavex and Alginoplast, respectively.
Conclusions
Digital dental models can be obtained from CBCT scans of alginate impressions without sending them to a remote laboratory. However, the impressions need to be scanned within 24 hours; otherwise, dimensional changes lead to errors that exceed the error of measurement.
Highlights
- •
Digital dental models can be obtained from cone-beam computed tomography (CBCT) scans of alginate impressions without sending them to a laboratory.
- •
The impressions must be scanned within 24 hours to prevent dimensional changes that lead to errors.
- •
Digital models and plaster casts can be obtained from 1 impression with a CBCT scanner to scan an alginate impression.
The use of three-dimensional (3D) images of the maxillofacial area provides accurate diagnostic information based on accurate visualization of anatomic structures and enables clinicians to establish precise treatment plans. Although cone-beam computed tomography (CBCT) images can provide excellent skeletal representations, detailed dental and interocclusal data cannot be obtained. The image quality obtained from CBCT is insufficient for a precise representation of the teeth; hence, the dental part in the CBCT image needs to be replaced with another imaging modality to produce a precise craniodental model.
Although the authors of most trials have used optical or laser-scanned dental images as a substitute for the dentition, Swennen et al introduced a technique to augment the virtual skull model with direct scanning of alginate impressions. Rangel et al also used CBCT-scanned alginate impressions to integrate digital dental casts into CBCT scans. With the CBCT-scanned alginate impression image, it was possible to fabricate a composite skull model in a computerized virtual environment, eliminating the need for plaster dental models.
As a method to obtain digital dental models without pouring plaster, digital impressions from intraoral scanning has been introduced. However, the accuracy of the intraoral scan data has not yet achieved consensus among professionals, especially when scanning is done in vivo, whereas scanning of plaster models in vitro shows relatively reliable accuracy. Furthermore, intraoral scanning still requires a long time to scan the entire dentition, although some studies have demonstrated a reduction in the scanning time. Grunheid et al reported that alginate impressions are still the preferred method with respect to chair time and patient acceptance in their study assessing the time and patient acceptance of an intraoral scanner. In case of successive laboratory work requiring the actual dental model such as for fabrication of indirect bonding trays, additional 3D printing should be performed to produce the physical model from the virtual images. With the use of the CBCT-scanned alginate impressions, both the digital model and the actual plaster cast can be obtained with a single impression; this results in a significant reduction in the clinical workload, particularly in clinics equipped with CBCT scanners.
If a CBCT-scanned alginate impression is used as a valid alternative to other digital model systems, the dimensional stability of the impressions needs to be evaluated and confirmed. Naidu et al reported that tooth width measurements and Bolton analyses of the digital models fabricated by CBCT scanning of alginate impressions were as reproducible as those of plaster models by digital calipers. White et al studied 16 sets of maxillary and mandibular vinyl polysiloxane and alginate impressions that were converted into CBCT scanned dental models to evaluate the accuracy of their intra-arch and interarch measurements. The results indicated that digital orthodontic models from CBCT-scanning of both alginate and vinyl polysiloxane impressions provided dimensionally accurate representations of intra-arch relationships for orthodontic evaluations. Wiranto et al assessed the validity of digital models obtained from CBCT scanning of alginate impressions in the tooth width measurements in 22 subjects and concluded that tooth width measurements on the digital models did not differ significantly from those on the plaster models.
On the other hand, Torassian et al reported that digital models produced from CBCT scanning of alginate impressions showed dimensional changes at 72 hours regardless of the type of materials, in their study on the stability of digital models fabricated from 2 traditional alginate materials and 2 alginate substitutes. Although dimensional changes were found in the impressions, they could not determine when the changes occurred during their experimental time period because the impressions were sent to a laboratory for scanning. No published studies have evaluated the dimensional accuracy of digital models on a consecutive-hour basis after the impressions. The purpose of this study was to investigate the dimensional accuracy of digital dental models from the CBCT scans of alginate impressions according to the time elapsed after the impressions were taken.
Material and methods
Twenty adults (8 men, 12 women; mean age, 26.5 years) with normal occlusion and no missing teeth were enrolled in this study. All subjects provided informed consent to participate.
Two impression materials, Cavex Impressional (Cavex Holland, Haarlem, The Netherlands) and Alginoplast (Heraeus Kulzer, Hanau, Germany), were used according to the manufacturers’ instructions. An impression of the maxillary arch of each subject was taken using a plastic impression tray (President Impression Tray System, Coltène/Whaledent, Altstätten, Switzerland). The excess area over the impression tray was trimmed without damaging the cervical areas of the dentition. Excess moisture on the surface of the impression was removed by gentle air drying. The impression was then placed in a plastic container lined on the bottom with a paper towel moistened with distilled water at room temperature and sealed with a lid. To control the amount of moisture in the plastic container, each towel was equally saturated with distilled water.
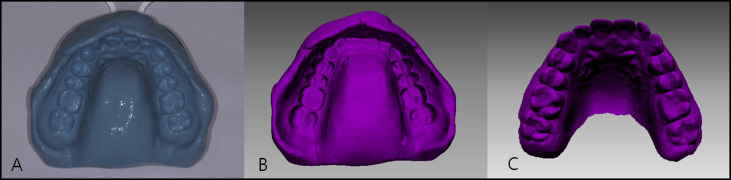
All alginate impressions were scanned immediately after impression-taking and after 12, 24, 36, 48, 60, and 72 hours with a CBCT scanner (Alphard Vega, Asahi Roentgen, Kyoto, Japan) under the following conditions: 80 kV, 5 mA, 0.2 × 0.2 × 0.2-mm voxel size, and 102 × 102-mm field of view. The digital imaging and communication in medicine (DICOM) file obtained with CBCT was reconstructed into 3D images and then converted to the stereolithography format using a 3D imaging program (Vworks version 4.0; CyberMed, Seoul, Korea) with identical Hounsfield units (−175) for each image. Then these images were imported into a 3D reverse engineering software program (Rapidform 2006; Inus, Seoul, Korea). The negative form of the alginate impression image was changed into the positive form using the “reverse normal” function of the program to produce a digital dental model ( Fig 1 ).
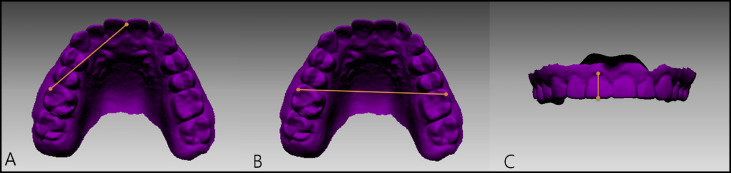
Using the image scanned immediately after impression-taking as the control, all images taken according to the time elapsed were reoriented to obtain a consistent 3D orientation with the “surface registration” function in the program. To evaluate the dimensional accuracy of each image, linear measurements were made on the digital models in the anteroposterior, transverse, and vertical dimensions. The anteroposterior dimension was evaluated by measuring the incisor-to-molar distance from the mesiobuccal cusp tip of the maxillary right first molar to the maxillary midline. The transverse dimension was measured using the intermolar width, the line between the mesiobuccal cusp tips of the maxillary right first molar and the maxillary left first molar. The vertical dimension was evaluated using incisor height, which is measured from the incisal edge at the midline of the maxillary right central incisor to the gingival margin ( Fig 2 ).
Statistical analysis
To assess the measurement errors, 20 images (10 Cavex impressions and 10 Alginoplast impressions) were selected randomly, and the measurements were made twice at an interval of 2 weeks by an operator (S-M.L.). The method errors of double registrations of all the measurements were calculated with Dahlberg’s formula as follows:
where d is the difference between the 2 measurements and n is the number of subjects. The errors were 0.29 mm for incisor-to-molar distance, 0.29 mm for intermolar width, and 0.27 mm for incisor height.
Means and standard deviations of the measurements were calculated for each material for each time period. Two-way analysis of variance (ANOVA) was carried out to evaluate the impacts and interactions of the materials and the time elapsed on the measurements. Means and standard deviations of the changes in measurements according to time elapsed were calculated. The changes in the measurement errors were assessed to evaluate the time point at which clinically relevant differences started to occur. All statistical analyses were carried out using SPSS software (version 20.0; IBM, Armonk, NY).
Results
Means and standard deviations of the measurements taken immediately after the impressions and at 12, 24, 36, 48, 60, and 72 hours later are given in Table I . The results showed a gradual decrease in the measurement values with the time elapsed, indicating that alginate materials underwent dimensional shrinkage over time. The results of the 2-way ANOVA showed significant differences on impression material ( P <0.001) and time elapsed ( P <0.001), whereas there was no significant material and time interaction ( P >0.05) ( Tables I and II ).


