Introduction
The introduction of digital cast models is inevitable in the otherwise digitized everyday life of orthodontics. The introduction of this new technology, however, is not straightforward, and selecting an appropriate system can be difficult. The aim of the study was to compare 4 orthodontic digital software systems regarding service, features, and usability.
Methods
Information regarding service offered by the companies was obtained from questionnaires and Web sites. The features of each software system were collected by exploring the user manuals and the software programs. Replicas of pretreatment casts were sent to Cadent (OrthoCAD; Cadent, Carlstadt, NJ), OthoLab (O3DM; OrthoLab, Poznan, Poland), OrthoProof (DigiModel; OrthoProof, Nieuwegein, The Netherlands), and 3Shape (OrthoAnalyzer; 3Shape, Copenhagen, Denmark). The usability of the programs was assessed by experts in interaction design and usability using the “enhanced cognitive walkthrough” method: 4 tasks were defined and performed by a group of domain experts while they were observed by usability experts.
Results
The services provided by the companies were similar. Regarding the features, all 4 systems were able to perform basic measurements; however, not all provided the peer assessment rating index or the American Board of Orthodontics analysis, simulation of the treatment with braces, or digital articulation of the casts. All systems demonstrated weaknesses in usability. However, OrthoCAD and 03DM were considered to be easier to learn for first-time users.
Conclusions
In general, the usability of these programs was poor and needs to be further developed. Hands-on training supervised by the program experts is recommended for beginners.
Highlights
- •
We compared 4 digital software systems regarding services, features, and usability.
- •
All 4 systems were similar regarding services and features.
- •
In general, the usability of these programs was poor and needs to be further developed.
- •
Hands-on training supervised by experts of the programs is recommended for beginners.
In many areas of health care, there is a shift toward digitization of patient information and data. Orthodontics is no exception. Medical records, x-rays, and photographs are just a few examples. Study models are central to orthodontic diagnosis, treatment planning, and evaluation. The introduction and use of digital models is inevitable in the otherwise digitized everyday life of orthodontics. Easy and effective storage, access, durability, transferability, and diagnostic versatility have been presented as advantages. Moreover, it is possible to communicate with colleagues and patients with virtual images that can be printed and e-mailed without effort. Clinicians could use the systems for marketing their clinics by showing prospective patients that the office is at the forefront of technology, with no up-front investment required. The systems make it possible to superimpose with other digital casts or to fuse with digital x-rays and digital photos. The first system for digital evaluation was introduced to the market in 2001. Since then, several systems have been marketed. Commercially available digital cast models can be produced by either direct or indirect techniques. Direct methods use interior scanners, and indirect methods use either laser scanning or computed tomography imaging of the impressions or plaster models. Subsequently, the scans are converted into digital images that are stored on the manufacturer’s servers. The models are then available for downloading by the account holder, and the manufacturer provides software for routine measurement. There is doubt, however, that these 2-dimensional computer screen systems can provide as much information as the hands-on 3-dimensional plaster models in terms of diagnosis, treatment planning, and evaluation. So far, the following systems have been evaluated almost exclusively regarding reliability and validity: Cecile, e-models, Orametrix, OrthoCAD, DigiModel, O3DM, and OrthoAnalyzer. Studies have demonstrated that even though the reliability of the systems is not ideal for research, it is adequate for clinical use. However, the introduction of this new technology is not straightforward, and selecting an adequate system may be difficult. Research has shown that to facilitate the shift in technology, manufacturers need to provide appropriate features and services, and their products should be easy to use. However, a more thorough comparison of various digital software systems used in orthodontics has not been done. The aim of this study was to compare 4 digital software systems regarding (1) service and support provided by the manufacturer, (2) features of the program, and (3) usability of the program.
Material and methods
The 4 orthodontic digital software systems evaluated were OrthoCAD (version 3.5.0; Cadent, Carlstadt, NJ), O3DM (version 3.2; OrthoLab, Poznan, Poland), Digimodel (version 2.2.1; OrthoProof, Nieuwegein, The Netherlands), and OrthoAnalyzer (version 1.5; 3Shape, Copenhagen, Denmark). Duplicates of pretreatment casts from patients at the Department of Orthodontics at the University of Gothenburg in Sweden were sent to these 4 companies for scanning and to subsequently be available in a digital format on a computer at the clinic.
Information regarding services provided from the companies—time until delivery, cost, technical requirements, and so on—was obtained from their Web sites. If additional information was needed, the manufacturer was contacted.
The features offered by each software system were collected from user manuals and by browsing the software programs. If additional information was needed, the manufacturer was contacted.
The “enhanced cognitive walkthrough” method was used to evaluate usability. Theoretically, the enhanced cognitive walkthrough focuses on ease of learning by exploration. This means that a user tries to complete a task using a trial-and-error technique. While the user performs the sequence of actions to accomplish the task, the method simulates the user’s cognitive processes. This determines whether the user’s background knowledge, together with hints from the interface, will lead to a correct sequence of goals and actions.
Practically, enhanced cognitive walkthrough is a method in which predefined tasks are performed by domain experts (in this study, A.W., M.R., S.P., A.B.), supervised by evaluators (in this case, experts in human-computer interactions [W.T., O.T.]).
In our study the 4 domain experts (A.W., M.R., S.P., A.B.) had much experience in orthodontic diagnosis and evaluation with an otherwise basic knowledge of computers. They had only limited experience in orthodontic measurements using digital analysis. The selection of tasks was based on the intended use: ie, measurements significant for orthodontic diagnosis and treatment planning such as opening up a patient file, viewing the casts from different angles, measuring overjet and overbite, and analyzing spaces.
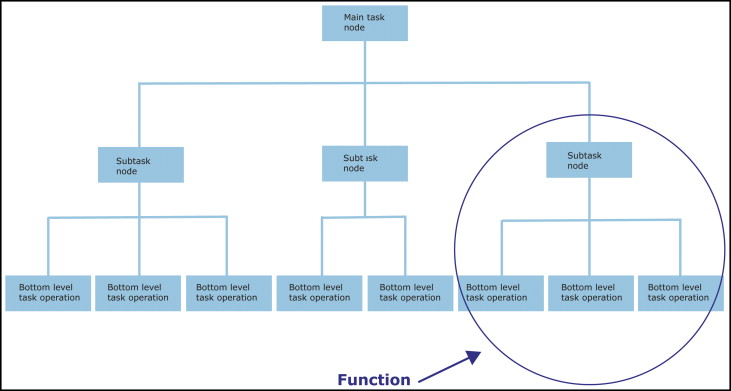
To evaluate usability, a 2-level question process is used. Level 1 is for function: ie, a sequence of actions comprising the tasks ( Fig 1 ). Level 2 is for the operations: ie, each step in a function ( Fig 2 ). The program’s or interface’s capability to capture the user is studied in level 1. In level 2, the user’s ability to perform the function correctly is studied. The analysis starts with the evaluator asking questions on level 1 for the whole function. Then the analysis continues with the operations. The underlying operations of a given node are analyzed in whole before the analysis continues in the next operation ( Fig 3 ).
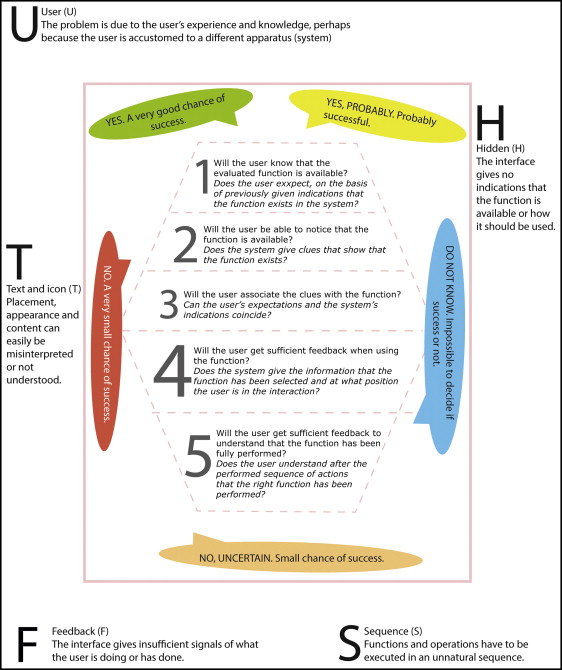
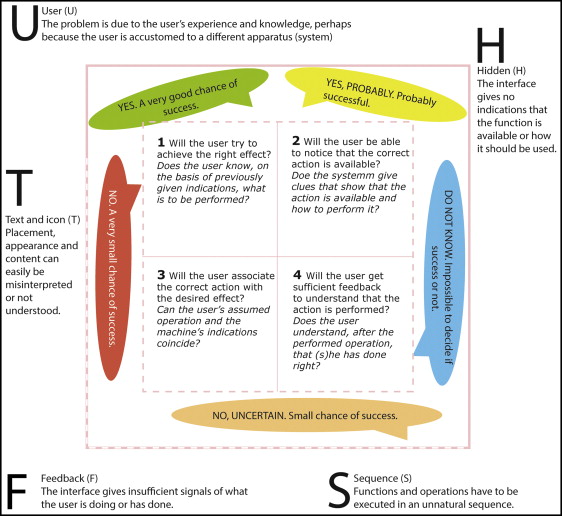
The questions are answered and graded (grades 1-5) as well as justified for each grade. The grading represents the different levels of success. The justifications are termed failure or success stories, and they describe the assumptions underlying the choice of grades: eg, whether the user can understand a text message or a symbol. The grade ranks are supposed to represent different problems in the interface: ie, the seriousness of the problem. This type of grading is used to determine what is most important to modify when redoing an interface. In the analysis process, the question is answered, assuming that the preceding questions are answered “yes” (grade 5).
The usability problem is the factor that prevents the user from accomplishing the action accurately. If the seriousness of the problem has been graded 1 to 4, it implies that there is a usability problem. This problem then needs to be described in a failure or a success story.
The problems found are subsequently categorized by type with a description of the problem and the failure stories. The problems vary with the user interface and the user’s task. Different problem types are described in Figures 1 and 2 .
In addition, the legibility and relevance of the logo to the representation of the systems were compared.
Results
The results demonstrated that all companies require alginate or silicone impressions, good-quality bite registrations of wax or silicone, and disposable trays. If needed, a plaster model can be made from the impression at some additional cost. Not all companies offer laboratory integration. Time until delivery of the digital casts and costs are similar, and costs are also similar to the cost of a regular plaster model ( Table I ). The services provided by the instruction materials from the companies are shown in Table II .
| OrthoAnalyzer | DigiModel | OrthoCAD | O3DM | |
|---|---|---|---|---|
| Cost | 30-35€ ($36-$43 USD) | 20€ ($25 USD) | 24€ ($30 USD) | 29€ ($35 USD) |
| Time until delivery | – | 24 hours | 48 hours | 48 hours |
| Requirements | Impression Plaster model Intraoral scan |
Impression Plaster model |
Impression Plaster model Intraoral scan |
Impression Plaster model |
| Impression material | PVS Alginate |
PVS Alginate |
PVS | PVS Alginate |
| Bite registration | PVS Wax |
PVS Wax |
PVS | Wax |
| Trays | Disposable | Disposable | Disposable | Disposable |
| Plaster/plastic model fabrication | Yes | Yes | Yes | Yes (18.2-25.47 euro) |
| Scanning technology | LED-laser | CT scanner | Laser | 3D scanner using laser beam |
| Digital model size | 3 MB | 4-5 MB | 3 MB | 3-4 MB |
| Software cost | Free | Free | Free | Free |
| Software size | 650 MB | 74 MB | 8 MB | 38.07-54.10 MB |
| File of digital model | Always available | Up to 14 years | Never delete file | |
| Laboratory integration | Yes | Yes | No | Yes |
| Compatibility with patient’s information system | Yes | Yes | Yes | Yes |
| Size (number of pages) | Content | Step-by-step instruction for a specific task | |
|---|---|---|---|
| OrthoCAD | 34 | The manual is not about the interface of the system but about integrating the system into the work practice and PVS impression. | Yes, but only 4 pages describing the process of approval of a cast. |
| DigiModel | Primarily online help divided into chapters that can be browsed (it was possible to print the online user guide). | Illustration of available functionality with images and step-by-step instructions about the interface. | No, mostly description of menu bars, panels, and icons. The descriptions are not organized into tasks. |
| OrthoAnalyzer | 114 | Illustration of available functionality with images and step by step instructions about the interface. | Yes. |
| O3DM | 167 | Illustration of available functionality with images and step-by-step instructions about the interface. | Yes, in the manual, important objects of user interface are marked in images with red arrows and circles. |
All 4 systems can perform basic measurements such as overbite, overjet, tooth size, space analysis, Bolton analysis, and arch length. The systems can show views of the digital cast in different planes; map occlusal contacts; make free measurements from point to point, point to plane, or plane to plane; and measure tooth movements in different planes. However, not all systems can provide the peer assessment rating index or the American Board of Orthodontics analysis, simulation of the treatment with braces, or digital articulation of the casts ( Table III ).
| OrthoAnalyzer | DigiModel | OrthoCAD | O3DM | |
|---|---|---|---|---|
| Virtual setup | Yes | Yes | Yes | Yes |
| Articulation | Yes | Yes | No | Yes |
| Superimposition | Yes | Yes | No | Yes |
| PAR index | No | Yes | No | Yes |
| Indirect bonding | Yes | Yes | Yes | Yes |
| Windows or Macintosh | Windows | Both | Windows | Both |
Task 1, opening up a patient file, was done through selecting an option in the main menu bar. All systems except OrthoAnalyzer have the menu option “file.” OrthoCAD, DigiModel, and 03DM refer to the patient as a “file.” File is a technical term showing the underlying software structure. The user’s mental model of a task is to access information about a specific patient’s model.
The number of issues for this task was the least for OrthoCAD and the greatest for OrthoAnalyzer. The issues could mainly be called “text and icon” and “hidden.” It could be concluded that for task 1, OrthoCAD, 03DM, and DigiModel were more usable than OrthoAnalyzer ( Table IV ).
| System | User | Text and icon | Hidden | Feedback | Sequence | Total |
|---|---|---|---|---|---|---|
| OrthoCAD | 0 | 0 | 0 | 0 | 0 | 0 |
| DigiModel | 0 | 1 | 1 | 0 | 0 | 2 |
| OrthoAnalyzer | 0 | 1 | 1 | 0 | 3 | 5 |
| O3DM | 0 | 1 | 1 | 0 | 0 | 2 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


