Introduction
The purposes of this study were to analyze the variations in dental arch dimensions of a large representative sample of adolescent Kuwaitis with untreated almost ideal occlusion and to test the validity of proposed expansion indexes and multivariate linear regression with inclusion of lateral and posteroanterior cephalometric parameters for estimation of dental arch width.
Methods
Study models and both lateral and posteroanterior cephalograms of 143 Kuwaitis, aged 13 to 14 years, clinically diagnosed with untreated almost ideal occlusion during screening of a population-based sample, were examined. Maxillary and mandibular arch dimensions were measured by using a digital caliper accurate to 0.01 mm, and cephalometric parameters were measured electronically.
Results
All dimensions were greater in boys than in girls ( P <0.001) and demonstrated wide individual variations. Maxillary arch-width estimates according to 3 proposed expansion indexes differed from the actual dimensions ( P <0.001), with more than 60% of the dimensions having discrepancies greater than 1.0 mm and explained variances from 0.12 to 0.20. Multivariate linear regression with inclusion of cephalometric parameters provided better estimates, with explained variances from 0.29 to 0.44.
Conclusions
The tested expansion indexes provide poor estimates of maxillary arch widths, with low explained variances. Multivariate linear regression provides better estimates, with moderate explained variances.
Increases in transverse dental arch dimensions are associated with arch perimeter gains. Maxillary expansion has therefore been recommended as a suitable alternative to premolar extraction, particularly in patients with narrow dental arches. Attempts have been made to establish guidelines for lateral expansion in orthodontic patients. Pont proposed a normative index, based on the assumption that the summed width of the maxillary incisors was similar to 80% of the distance between the distal ends of the occlusal grooves of the maxillary first premolars and similar to 64% of the distance between the central fossae of the maxillary first molars in subjects with ideal, well-aligned dentitions. Schwarz and Grätzinger modified Pont’s index according to facial type, adding 6 vs 12 mm to the summed width of the maxillary incisors as a guide to determine ideal interpremolar and intermolar widths in dolichofacial or high-angled patients, 7 vs 14 mm in mesofacial or normally proportioned patients, and 8 vs 16 mm in brachyfacial or low-angled patients. Howe et al later proposed a simplified rule of thumb, suggesting that ideal intermolar widths measured at the midpoint of the lingual surfaces of the maxillary first molars are 37.4 mm in males and 36.2 mm in females. More recent guidelines are based on a posteroanterior cephalometric analysis, recommending expansion for maxillomandibular discrepancies larger than 5 mm relative to Ricketts’ norm of 19.6 mm for adults, or larger than 21.3 mm in young adolescents after adjustment for magnification.
The above indexes and recommendations are proposed diagnostic aids for the determination of the amount of maxillary expansion that can be performed to gain dental arch perimeter in an orthodontic patient with a space deficiency. However, the clear consequence that a similar transverse expansion will be needed in the mandibular arch, and whether such expansion might be a challenge to stability of the orthodontic treatment result, was not addressed. Longitudinal growth studies have demonstrated a minimal potential for increases in mandibular dental arch dimensions after the establishment of the permanent dentition. In addition, postretention follow-up examinations have documented an association between treatment increase and postretention reduction in mandibular intercanine distance and a general tendency for altered mandibular arch forms to return toward their pretreatment shapes. Finally, a strong association has been detected between the postretention reduction in mandibular intercanine distance and the increase in mandibular incisor irregularity. A contradictory and more commonly accepted approach is therefore to minimize treatment-induced changes in mandibular arch form unless they are necessary for crossbite correction, to treat arch-length deficiency with premolar extraction unless mandibular incisor proclination is warranted, and to adjust the shape of the maxillary arch to that of the mandibular arch.
Pont and Schwarz and Grätzinger did not describe the samples forming the basis for their indexes. Howe et al compared a group of 50 patients with crowding with a group of 54 subjects with Class I normal occlusions and little or no crowding. However, the samples were of various ages and were not derived from screening representative populations according to objective criteria. Selection biases according to personal concepts of what constitutes an ideal arch form can therefore not be ruled out. The actual sample used by Ricketts to develop his age-specific norms for maxillomandibular differences was not described. For either expansion index or analysis to be valid, ideal untreated occlusions should have maxillary arch widths close to the predicted widths.
Subjects with acceptable occlusion and no history of orthodontic treatment have demonstrated significant associations between actual and predicted arch widths according to the definition and index of Pont. However, the explained variances were low, and less than 30% of the subjects had arch-width dimensions within 1 mm of the predicted values. Few attempts have been made at testing the validity of the index of Schwarz and Grätzinger and the rule of thumb of Howe et al, with only 43 adolescents with untreated ideal occlusion. Moreover, information is limited regarding the relative accuracy of predictions according to these 3 indexes.
Alvaran et al concluded that a multivariate model including anthropometric facial height and width measurements enhanced the reliability of the predictions. However, their lack of access to posteroanterior cephalograms precluded inclusion of the interjugular width, which is a key parameter in the analyses recommended by Vanarsdall and Ricketts. Moreover, lack of access to lateral cephalograms precluded inclusion of the mandibular plane angle. Recent findings suggest that dental arch width varies according to the steepness of the mandibular plane. The purposes of our study were to analyze the variations in dental arch dimensions in a large, representative group of adolescents with natural development of almost ideal occlusion and to test the relative accuracy of arch-width predictions according to the indexes of Pont, Schwarz and Grätzinger, and Howe et al, and multivariate regression with inclusion of relevant vertical and transverse cephalometric parameters. The findings might indicate to which degree the decision to treat an arch-length deficiency with bimaxillary expansion can be based on objective criteria.
Material and methods
After approval by the ethics committee of Kuwait University, Faculty of Dentistry, and authorization by the Research Department of the Kuwaiti Ministry of Education, 13- to 14-year-old eighth-grade students were screened during regular school hours. The students were informed about their rights to participate in the study, and each school principal provided a well-lit room for the examinations. Kuwaiti nationals aged 13 to 14 years with no history of orthodontic treatment and subjectively diagnosed with almost ideal occlusion, defined as perfect intercuspation and posterior tooth alignment with no transverse discrepancy, no detectable lateral shift, anterior shift less than 2 mm, no midline deviation, positive overjet less than 3.5 mm, positive overbite less than two thirds overlap of the maxillary to the mandibular incisors, arch-length excess less than 2 mm in either arch, and anterior tooth irregularity less than 3.5 mm in either arch were invited to participate in clinical and radiographic examinations. With written parental consent, 82 boys (mean age, 13.27 ± 0.42 years) and 80 girls (mean age, 13.21 ± 0.43 years) were examined. Based on a careful examination of the study models, 19 subjects were excluded, due to either incomplete eruption of premolars, severely decayed first molars, premolar rotations, retained deciduous molars, or incisor irregularity. The final sample therefore consisted of 69 boys and 74 girls.
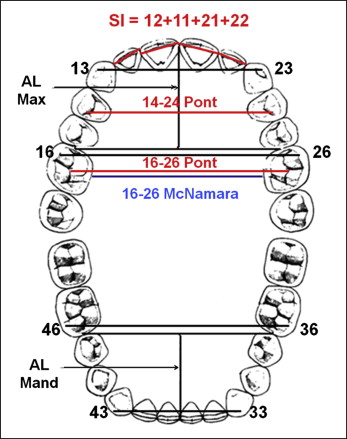
Impressions were made of each dental arch by using alginate and impression trays coated with synthetic fluorine-containing resin. The impressions were poured in orthodontic stone and trimmed according to the wax bite registration in centric occlusion. Model measurements were made by using a digital caliper accurate to 0.01 mm. The widths of teeth 11, 12, 21, and 22 (FDI numbering) were measured as the widest mesiodistal dimension, the widths of 13 to 23 and 33 to 43 as the distance between the cusp tips, and the widths of 16 to 26 and 36 to 46 as the distance between the mesiobuccal cusp tips ( Fig 1 ). Maxillary and mandibular arch lengths were measured as the distance from the contact point between the central incisors to the line connecting the mesial contact points of the first molars ( Fig 1 ). The distances between the distal ends of the occlusal grooves of teeth 14 and 24 and between the central fossae of the occlusal surfaces of teeth 16 and 26 were measured as defined by Pont, whereas the distance between the midpoints of the lingual surfaces of teeth 16 to 26 was measured according to the index of Howe et al ( Fig 1 ).
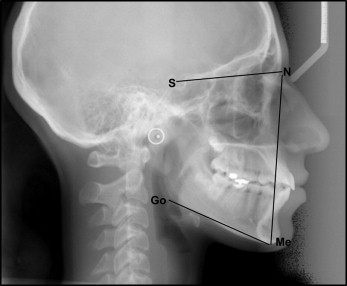
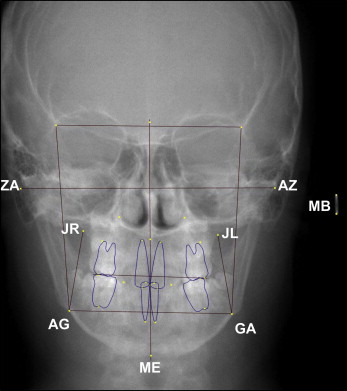
Digital lateral and posteroanterior cephalograms were made with the teeth in centric occlusion at a focus-to-object distance of 150 cm and an object-to-receptor distance of 20 cm with a cephalostat (Planmeca publication 688169, version 5; Planmeca, Helsinki, Finland). Each subject was placed in the head holder and asked to look straight forward before the nasal positioner was adjusted. The reference points were identified directly on the digital lateral and posteroanterior cephalometric images. Anterior facial height was defined as the distance N-Me and mandibular plane angle as the angle SN/Me-Go ( Fig 2 ). The interzygomatic width was defined as the distance between the most lateral aspects of the centers of the right and left zygomatic arches, the interjugular width as the distance from the right to the left intersections between the zygomatic and alveolar processes, the intergonion width as the distance between the lateral and inferior borders of the right and left antegonial notches, and the maxillomandibular discrepancy as intergonion width minus interjugular width ( Fig 3 ). The dimensions were calculated electronically by using the Dolphin software package (version 9; Dolphin Imaging and Management Solutions, Chatsworth, Calif), adjusting the linear readings to the actual subject dimensions according to the millimeter ruler on the lateral cephalograms ( Fig 2 ) and the dimension of the metal bar on the posteroanterior cephalograms ( Fig 3 ).
The reproducibility of the measurements was assessed by statistically analyzing the difference between double measurements taken at least 1 month apart on 10 randomly selected sets of study models and lateral cephalograms. The entire procedure for the computer-generated measurements was repeated. The error of the method was calculated from the equation:
where D is the difference between duplicated measurements and N is the number of double measurements. The errors ranged from 0.03 (maxillary intermolar width) to 0.31 (mandibular intermolar width) for the study model measurements and were 1.25 for N-Me, 0.74 for SN/Me-Go, 0.88 for interzygomatic width, 0.91 for intergonion width, and 0.91 for interjugular width. The Pearson R values between the first and second measurements were all greater than 0.98 ( P <0.001) for the study model measurements and greater than 0.90 ( P <0.001) for the cephalometric measurements.
Statistical analysis
For each model, the widths of the 4 maxillary incisors were summed to 1 value ( Fig 1 ). Arch-width prediction according to the index of Pont was performed by dividing the summed width of the maxillary incisors by 0.80 to estimate the 14 to 24 distance, and by dividing the summed width by 0.64 to estimate the 16 to 26 distance. Facial type was classified according to the facial index and categorized as dolichocephalic (leptoprosopic) for N-Me/interzygomatic width of ≥0.900, as mesocephalic for N-Me/interzygomatic width of 0.849 to <0.900, and as brachycephalic (euryprosopic) for N-Me/interzygomatic width of ≤0.850. The respective predicted 14 to 24 and 16 to 26 widths according to the index of Schwarz and Grätzinger were calculated as the summed width of the maxillary incisors +6 and +12 for dolichocephalic facial types, as the summed width +7 and +14 for mesocephalic types, and as the summed width +8 and +16 for brachycephalic types. Descriptive statistics were performed for all measured and calculated dental arch parameters. Sex differences associated with the measured and calculated width dimensions were evaluated by using independent t tests. Pearson correlation measurements ( R ) were used to quantify the statistical associations. Finally, univariate logistic regression was used to test the associations between the measured dental arch-width dimensions and the summed width of the maxillary incisors as well as the parameters calculated from the lateral and posteroanterior cephalograms. After that routine, forward stepwise multiple logistic regression was used to develop prediction models for the measured dental arch-width dimensions. Variables were successively entered into the models if their effects were significant at P <0.05. At each step, the variable with the lowest P value was included. Previously entered variables were excluded if their effects were no longer significant ( P >0.05) upon inclusion of a new variable. The final models were determined when no remaining variables had a significant effect ( P >0.05). All statistical analyses were carried out by using SPSS software (version 17; SPSS, Chicago, Ill).
Results
The ranges of all measured and calculated dimensions were large, and every dimension was greater ( P <0.001) in boys than in girls ( Table I ). Associations were found ( P <0.001) between maxillary arch length and both the widths of 13 to 23 ( R = 0.33) and 16 to 26 ( R = 0.55), as well as between mandibular arch length and the width of 33 to 43 ( R = 0.48). However, mandibular arch length was not associated with the width of 36 to 46 ( R = 0.14, P = 0.10). Finally, associations were detected ( P <0.001) between the widths of 13 to 23 and 33 to 43 ( R = 0.72), between the widths of 16 to 26 and 36 to 46 ( R = 0.90), and between maxillary and mandibular arch lengths ( R = 0.84).
| Boys (n = 69) | Girls (n = 74) | Total (n = 143) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Min | Max | Mean ± SD | Min | Max | Mean ± SD | Min | Max | |
| SI | 31.48 ± 1.95 | 25.80 | 39.10 | 30.65 ± 1.70 | 26.70 | 34.40 | 31.05 ± 1.87 | 25.80 | 39.10 |
| 13-23 | 34.91 ± 1.86 | 30.40 | 39.00 | 33.63 ± 1.60 | 29.10 | 37.40 | 34.25 ± 1.84 | 29.10 | 39.00 |
| 14-24 Pont | 38.42 ± 2.12 | 34.10 | 42.50 | 36.63 ± 1.73 | 32.20 | 40.00 | 37.50 ± 2.12 | 32.20 | 42.50 |
| 14-24 Pont est | 39.35 ± 2.44 | 32.25 | 48.88 | 38.31 ± 2.13 | 33.38 | 43.00 | 38.81 ± 2.34 | 32.25 | 48.88 |
| 14-24 Schwarz est | 38.55 ± 2.24 | 32.80 | 47.10 | 37.71 ± 1.79 | 33.70 | 41.70 | 38.11 ± 2.05 | 32.80 | 47.10 |
| 16-26 | 52.39 ± 2.48 | 47.40 | 57.80 | 50.31 ± 2.32 | 44.80 | 55.80 | 51.32 ± 2.61 | 44.80 | 57.80 |
| 16-26 Pont | 48.44 ± 2.34 | 44.00 | 53.00 | 46.11 ± 2.43 | 40.00 | 54.00 | 47.23 ± 2.65 | 40.00 | 54.00 |
| 16-26 Howe | 36.08 ± 2.28 | 31.20 | 40.30 | 34.95 ± 2.12 | 29.10 | 40.20 | 35.49 ± 2.26 | 29.10 | 40.30 |
| 16-26 Pont est | 49.19 ± 3.05 | 40.31 | 61.09 | 47.88 ± 2.66 | 41.72 | 53.75 | 48.52 ± 2.92 | 40.31 | 61.09 |
| 16-26 Schwarz est | 45.61 ± 2.77 | 39.80 | 55.10 | 44.81 ± 2.17 | 40.50 | 49.70 | 45.19 ± 2.50 | 39.80 | 55.10 |
| Maxillary AL | 28.43 ± 1.65 | 24.90 | 32.10 | 27.45 ± 1.47 | 24.80 | 32.20 | 27.93 ± 1.63 | 24.80 | 32.20 |
| 33-43 | 26.72 ± 1.58 | 22.70 | 29.90 | 25.65 ± 1.41 | 23.10 | 29.90 | 26.16 ± 1.58 | 22.70 | 29.90 |
| 36-46 | 44.73 ± 2.33 | 40.00 | 50.00 | 42.87 ± 2.28 | 37.00 | 48.00 | 43.77 ± 2.48 | 37.00 | 50.00 |
| Mandibular AL | 23.80 ± 1.53 | 20.20 | 27.30 | 23.02 ± 1.36 | 20.30 | 25.80 | 23.40 ± 1.50 | 20.20 | 27.30 |
Estimated values for the 14 to 24 and 16 to 26 widths according to the Pont index were correlated with the measured distances ( R = 0.42 and 0.37, respectively; P <0.001) but larger than the measured distances ( P <0.001, Table I ). The maximum overestimations were 7.1 mm for the 14 to 24 width and 8.9 mm for the 16 to 26 width, with respective maximum underestimations of 4.0 and 5.8 mm. Totals of 14.7% and 18.2% of the respective estimated distances were at least 4.0 mm smaller or larger than the measured distances, whereas 37.0% and 27.3% were within 1.0 mm of the actual distances ( Table II ).
| x >4 mm | x >2 mm | x ±1 mm | x <2 mm | x <4 mm | |
|---|---|---|---|---|---|
| 14-24 Pont est | 14.7 | 31.5 | 37.0 | 4.2 | 0.0 |
| 16-26 Pont est | 16.8 | 38.5 | 27.3 | 11.9 | 1.4 |
| 14-24 Schwarz est | 7.1 | 22.1 | 42.1 | 8.6 | 0.7 |
| 16-26 Schwarz est | 0.7 | 6.4 | 26.5 | 45.7 | 19.3 |
| 16-26 Howe est | 9.8 | 37.8 | 28.0 | 5.6 | 0.0 |
Estimated values for the 14 to 24 and 16 to 26 widths according to the index of Schwarz and Grätzinger were correlated with the respective measured values ( R = 0.44 and 0.35; P <0.001). The estimated value for the 14 to 24 width was larger ( P <0.001) than the actual distance ( Table I ), with a maximum overestimation of 6.4 mm and a maximum underestimation of 4.6 mm. However, the estimated value for the 16 to 26 width was smaller ( P <0.001) than the actual distance ( Table I ), with a maximum overestimation of 4.5 mm and a maximum underestimation of 8.6 mm. Totals of 7.8% and 20.0% of the respective estimated distances deviated at least 4.0 mm from the measured distances, whereas 42.1% and 26.5% were within 1.0 mm of the actual dimensions ( Table II ).
The average boy and girl had a narrower 16 to 26 width as defined by Howe et al ( P <0.001) than the proposed respective averages of 37.4 and 36.2 mm ( Table I ). The maximum narrowing values were 6.2 mm for boys and 7.1 mm for girls, with maximum widenings of 2.9 and 4.0 mm, respectively. Only 28.0% of the subjects demonstrated actual distances within 1.0 mm of the stated averages ( Table II ), with 74.5% of the boys and 73.0% of the girls having distances narrower than the proposed averages.
Univariate linear regression showed that the summed width of the maxillary incisors, interjugular width, and interzygomatic width were associated with all measured arch-width dimensions ( Tables III-VII ), with explained variances ( R 2 ) ranging from 0.10 (14 to 24 width as defined by Pont in girls, Table VI ) to 0.35 (14 to 24 width as defined by Pont in boys, Table VI ) for the summed width of the maxillary incisors, from 0.07 (33 to 43 width in boys, Table VII ) to 0.30 (16 to 26 width as defined by Pont in boys, Table IV ) for interjugular width, and from 0.07 (33 to 43 width in boys, Table VII ) to 0.18 (16 to 26 width in girls, Table III ) for interzygomatic width. MP/SN was not associated with any width dimension ( P >0.05, Tables III-VII ). The effects of the remaining parameters varied among the width dimensions, with R 2 ranging from 0.00 to 0.30.
| R 2 | Univariate effect ± SE | P | R 2 | Multivariate effect ± SE | P | |
|---|---|---|---|---|---|---|
| Boys | 0.44 | |||||
| SI | 0.28 | 0.68 ± 0.13 | <0.001 | 0.50 ± 0.13 | <0.001 | |
| MP/SN | 0.00 | −0.03 ± 0.05 | 0.60 | |||
| JR-JL | 0.25 | 0.24 ± 0.05 | <0.001 | 0.18 ± 0.05 | <0.001 | |
| GA-AG | 0.04 | 0.10 ± 0.06 | 0.10 | |||
| (GA-AG) – (JR-JL) | 0.12 | −0.19 ± 0.06 | <0.01 | |||
| ZA-AZ | 0.08 | 0.09 ± 0.04 | <0.05 | |||
| N-Me | 0.01 | 0.04 ± 0.05 | 0.36 | |||
| N-Me/ZA-AZ | 0.03 | −6.25 ± 4.51 | 0.17 | |||
| Girls | 0.39 | |||||
| SI | 0.17 | 0.56 ± 0.15 | <0.001 | 0.31 ± 0.14 | <0.05 | |
| MP/SN | 0.00 | 0.02 ± 0.06 | 0.67 | |||
| JR-JL | 0.25 | 0.29 ± 0.06 | <0.001 | |||
| GA-AG | 0.29 | 0.24 ± 0.04 | <0.001 | 0.29 ± 0.06 | <0.001 | |
| (GA-AG) – (JR-JL) | 0.04 | 0.10 ± 0.06 | 0.11 | −0.15 ± 0.07 | <0.05 | |
| ZA-AZ | 0.18 | 0.15 ± 0.04 | <0.001 | |||
| N-Me | 0.05 | 0.10 ± 0.05 | 0.05 | |||
| N-Me/ZA-AZ | 0.05 | −11.59 ± 5.98 | 0.06 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


