Introduction
The purposes of this study were to investigate the dental arch changes after adenotonsillectomies in prepubertal children and to compare the dental arch dimensions of mouth-breathing and nasal-breathing children.
Methods
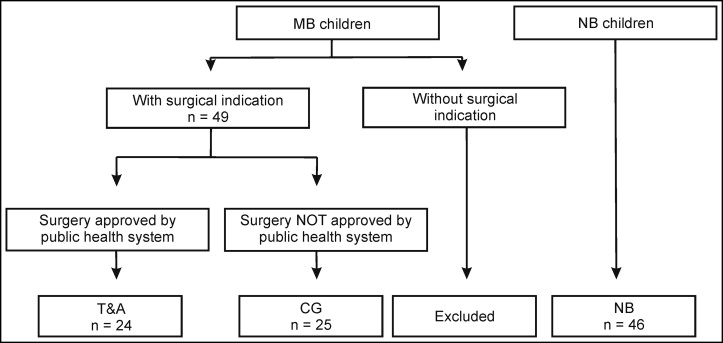
The sample included 49 prepubertal severely obstructed mouth-breathing children and 46 prepubertal nasal-breathing children. Twenty-four of the 49 mouth-breathing children had an adenotonsillectomy and composed the adenotonsillectomy subgroup. The 25 children in whom the mouth-breathing pattern was unchanged during the 1-year study period composed the control subgroup.
Results
The mouth-breathing children showed a deeper palatal vault, a larger mandibular width, and a larger mandibular arch length in comparison with the nasal-breathing children. After airway clearance, the adenotonsillectomy group showed a significant maxillary transverse width gain compared with the control subgroup. The control subgroup showed a significant deepening of the palatal height when compared with the adenotonsillectomy subgroup after 1 year.
Conclusions
The adenotonsillectomy subgroup had a significantly different pattern of arch development compared with the untreated controls. After adenotonsillectomy, the mouth-breathing children showed greater maxillary transverse development than did the controls. The palatal vault deepened in the untreated children. The mouth-breathing children showed a deeper palatal vault, a larger mandibular width, and a larger mandibular arch length in comparison with the nasal-breathing children.
The association between mouth breathing (MB) and facial morphology impairment is quite old. In past years, obstructive sleep apnea, the most extreme type of MB, has received significant attention by orthodontists; this has increased interest in this topic. Previous animal and clinical studies have provided evidence of the role of MB in abnormal dentofacial growth. The data showed that adaptive changes occur in the form and the size of the maxillary and mandibular dental arches in response to alterations in head, mandibular, and tongue positions. Alterations in the dental arch dimensions such as change in the depth of the palatal vault, decreased intercanine and molar distances, and changes in the position of the incisors are expected to follow changes in the mode of respiration from nasal to oral. Although such an assumption has a strong theoretical basis in physiopathology, some controversy remains, including whether MB is associated with dental arch deformities, and the effect of surgical normalization on breathing mode and dental arch development.
The literature suggests that normalization of the mode of respiration in children results in dentofacial growth similar to that of the nasal-breathing (NB) controls. It is well accepted that early removal of obstructive tissues in the upper airway during the prepubertal stage of development promotes a positive change in balanced facial growth. Cohort studies have found no differences in the dental arch morphology of young children treated with tonsillectomy and adenoidectomy, suggesting that the relationship between MB and dental arch dimensional changes is not easily predictable. Those studies had an NB control group or a small sample for the MB control group. A longitudinal study with an untreated MB control group would facilitate an understanding of the influence of MB and tonsillectomy and adenoidectomy on the dental arches in prepubertal children.
Since occlusal traits are associated with the mode of breathing, the purpose of this 1-year cohort study was to test, during the prepubertal stage, the null hypotheses that (1) the dental arch dimensional changes after tonsillectomy and adenoidectomy are similar to those observed in the untreated MB control subgroup and (2) there is no difference in the dental arch dimensions of MB and NB children.
Material and methods
The study protocol was approved by the ethics committee of the Pontifical Catholic University of Minas Gerais, Belo Horizonte, Brazil. Informed written consent was obtained from the parents before the subjects entered the study.
The sample involved dental casts of 95 prepubertal children (49 MB, 46 NB). All 95 children were in the late deciduous or early mixed dentition at baseline (T0). The median ages at T0 were 6.0 years (mean, 6.2 ± 1.7 years) in the MB group (65.3% boys) and 5.9 years (mean, 5.9 ± 1.3 years) in the NB group (45.6% boys). The ages ranged from 3.11 to 10.10 years at T0. The exclusion criteria were as follows: no history of previous orthodontic or orthopedic treatments, no lip or palate clefts, and no history of a persistent sucking habit at the beginning of the study.
The 49 MB children were selected from a larger project, which was undertaken to investigate the influence of MB on dentofacial growth. These children were consecutively referred by pediatricians or primary care physicians to the Outpatient Clinic for Mouth Breathers at the Federal University of Minas Gerais in Brazil, with the chief complaint of MB. They were systematically evaluated at 1 visit by a multidisciplinary team comprising otorhinolaryngologists, allergists, and orthodontists. Based on the clinical and endoscopic otorhinolaryngology examination performed at the first consultation by 2 authors (L.P.F. and H.M.G.B.), the upper airways were thoroughly examined, and the nasopharyngeal obstructions by adenoidal tissue were classified into the following 3 categories: mild (<50%), moderate (50%-75%), and severe (≥75%). Palatine tonsil hypertrophy was classified according to previously published criteria. Children with severe obstructions (nasopharynx obstruction ≥75% or tonsils with grades 3 and 4 according to Brodsky and Koch ) with an otorhinolaryngology surgery indication were included in this investigation. Of the 49 MB children, 30 had normal occlusion (Class I deciduous canine relationship, minimal overbite and overjet), and 19 subjects had a Class II relationship. Posterior crossbite was found in 14 MB children, and anterior open bite was diagnosed in 17 impaired subjects. The mean ANB angle was 5.5° ± 2.2°, and the mean SNB angle was 75.4° ± 3.6°. Twenty-four subjects from the 49 in the MB group, who had tonsillectomy and adenoidectomy, were followed for 1 year and comprised the tonsillectomy and adenoidectomy subgroup. The 25 MB children who did not have surgery during the 1-year observation period comprised the untreated control subgroup. No differences were found in the frequency of posterior crossbites or anterior open bites between the tonsillectomy and adenoidectomy and control subgroups. Those children were on the waiting list for authorization for tonsillectomy and adenoidectomy from the municipal health service, which, at the time of the sample collection (2006-2010), generally took more than 1 year for surgical approval because of high demand and low availability. During this waiting period, no children had any medical management (surgical or nonsurgical) that might have altered the soft-tissue inflammation of the airways. Figure 1 is a flowchart of the sampling process.
The NB children were selected from a growth study sample at the Pontifical Catholic University of Minas Gerais (ethics committee CAAE 2001/02) and had normal occlusion (Class I deciduous canine relationship, minimal overbite and overjet). The mean ANB angle was 5.2° ± 1.7°, and the mean SNB angle was 76.3° ± 4.2°. A parent of each child was questioned about the child’s medical history to exclude any subject with chronic MB, permanent snoring, and tonsillectomy or adenoidectomy. Nasal breathers with obvious hyperplasia of the tonsils and adenoids on the cephalometric images were excluded from further analysis.
The patients in each group were matched by chronologic age and stage of skeletal maturation, which was evaluated by the lateral cephalometric radiograph morphologic aspect of the cervical vertebrae C2, C3, and C4. All subjects were in cervical vertebrae stage 1 (prepubertal) at T0, were of the same ethnicity, and lived in the same metropolitan area at the time of the sampling process.
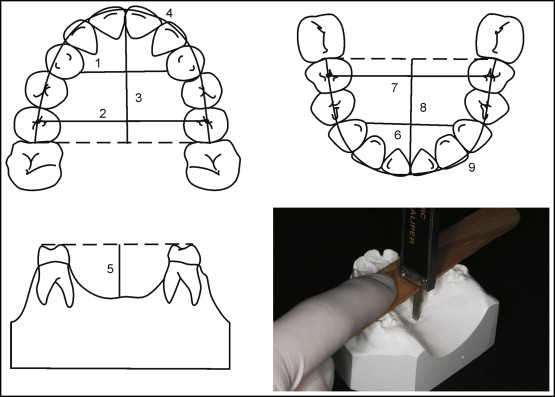
Study casts were taken from all 95 children at T0 and from the tonsillectomy and adenoidectomy and control children at the follow-up, 1 year ± 2 months later (T1). Their ages ranged from 5.1 to 12 years at T1. Nine dental arch dimension measurements were recorded by 1 examiner (A.C.P.C.) and are illustrated in Figure 2 , including the following: maxillary and mandibular intercanine widths, intermolar width, dental arch length, dental arch perimeter, and palatal depth.
To reduce the effect of accidental errors and improve reliability, the mean of 3 consecutive measurements, which were accepted only if they differed by less than 0.5 mm, was used for the calculations. The correlation coefficient (r) between the 3 measurements was greater than 0.96 for all variables.
The definition of each measurement is as follows.
- 1.
Maxillary and mandibular intercanine width: the distance (mm) between the most cervical lingual portion of the maxillary and mandibular right and left deciduous canine. The landmarks were placed at the gingival margin of the teeth on the assumption that the measurement is not affected by attrition or malposition of the teeth.
- 2.
Maxillary and mandibular intermolar width: the distance (mm) between the central fossae of the right and left deciduous second molars in both arches.
- 3.
Maxillary and mandibular dental arch length: the distance (mm) between the central incisors’ midpoints and the tangent line to the distal surface of the right and left deciduous second molars in both arches. The dental arch length denotes the sagittal dimension from the most anterior reference point to the posterior surface.
- 4.
Maxillary and mandibular dental arch perimeters: the contour of the dental arch (mm) measured from the distal surface of the left deciduous second molar to the distal surface of the right deciduous second molar passing over the central fossae of the deciduous molars, the tip of the deciduous canine, and the incisal edge of the incisors. The dental arch perimeter denotes the shape of the dental arch.
- 5.
Palatal depth: measured from the deepest point in the palate to a line connecting the mesiolingual tips of the deciduous second molars cusps. To record this, the tip of a digital caliper was inserted into the curved groove of a 1.74-mm-thick wooden tongue depressor, as shown in Figure 2 .
A digital caliper (4 in, model 47256; Cen-Tech, Pittsburgh, Pa), accurate to 0.001 mm, was used in the measurements. The evaluations were performed at T0 and repeated at T1. Measurements associated with exfoliated teeth were considered missing values for the subject.
To determine errors in the dental arch measurements, 52 randomly selected dental casts were remeasured by the same examiner at least 1 month later. The random errors were calculated using Dahlberg’s formula, and the systematic errors (bias) were assessed using the paired t test at P <0.05.
Statistical analysis
The data were analyzed using SPSS software (version 12.0; SPSS, Chicago, Ill). The systematic errors in the measurements did not exceed 0.02 mm and were thus considered to be of no further importance. The random errors ranged between 0.03 and 0.05 mm for the linear measurements. There were no statistically significant differences among the 3 measurements. The significance level was set at 5%. The Kolmogorov-Smirnov and Levene tests demonstrated normality and homoscedasticity, respectively, and thus the independent-sample t test was used.
Results
Four of the 9 measurements ( Fig 2 ) at T0 showed differences between the MB and NB groups. Statistically significant differences ( P <0.05) were observed between the MB and NB groups regarding palatal depth (MB, 14.60 mm vs NB, 13.87 mm), mandibular intercanine width (MB, 18.45 mm vs NB, 17.62 mm), mandibular second molar width (MB, 35.61 mm vs NB, 34.32 mm), and mandibular dental arch length (MB, 22.28 mm vs NB, 23.38 mm) ( Table I ). When the MB group was stratified into 2 groups, no statistically significant differences were found between the tonsillectomy and adenoidectomy and the control subgroups at T0 ( Table II ). Table III presents the dental arch measurements of the tonsillectomy and adenoidectomy and control subgroups. Paired t tests compared T0 and T1 in the tonsillectomy and adenoidectomy and control subgroups; independent t tests compared the tonsillectomy and adenoidectomy and control subgroups at T1. In the untreated children, 7 of 9 measurements had statically significant differences between T0 and T1. On the other hand, the tonsillectomy and adenoidectomy children showed differences from T0 to T1 in only 3 measurements. The dimensional changes in the dental arches of the tonsillectomy and adenoidectomy and the control subgroups between T0 and T1 were converted into percentages of the changes ( Figs 3 and 4 ) because the head size of children can vary even in the same developmental stage. The major results can be summarized as follows.
| Measurement (mm) | MB (n = 49) |
NB (n = 46) |
Independent t test | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | P value | |
| Maxillary intercanine width | 22.78 | 2.41 | 22.93 | 1.49 | 0.711 |
| Maxillary second molar width | 39.31 | 2.17 | 39.11 | 1.83 | 0.630 |
| Maxillary dental arch length | 26.18 | 2.17 | 26.38 | 1.58 | 0.616 |
| Maxillary dental arch perimeter | 75.69 | 5.70 | 75.46 | 3.48 | 0.813 |
| Palatal depth | 14.60 | 1.51 | 13.87 | 1.22 | 0.013 ∗ |
| Mandibular intercanine width | 18.45 | 1.84 | 17.62 | 1.38 | 0.016 ∗ |
| Mandibular second molar width | 35.61 | 1.96 | 34.32 | 1.81 | 0.001 ∗ |
| Mandibular dental arch length | 22.28 | 1.64 | 23.38 | 1.30 | 0.001 ∗ |
| Mandibular dental arch perimeter | 68.14 | 3.69 | 68.14 | 3.27 | 0.999 |
| Measurement (mm) | T & A (n = 24) |
CG (n = 25) |
Independent t test | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | P value | |
| Maxillary intercanine width | 22.71 | 2.32 | 22.84 | 2.54 | 0.847 |
| Maxillary second molar width | 38.93 | 2.02 | 39.67 | 2.29 | 0.240 |
| Maxillary dental arch length | 25.89 | 2.18 | 26.46 | 2.26 | 0.367 |
| Maxillary dental arch perimeter | 75.34 | 5.37 | 76.03 | 6.09 | 0.675 |
| Palatal depth | 14.40 | 1.41 | 14.81 | 1.62 | 0.368 |
| Mandibular intercanine width | 18.88 | 1.46 | 17.99 | 2.10 | 0.098 |
| Mandibular second molar width | 35.96 | 1.74 | 35.27 | 2.14 | 0.222 |
| Mandibular dental arch length | 22.13 | 1.60 | 22.41 | 1.70 | 0.552 |
| Mandibular dental arch perimeter | 67.82 | 3.44 | 68.45 | 3.97 | 0.562 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


