Figure 3.7 Patient’s pain location, right masseter muscle.

Figure 3.8 Patient showing pain location, right temporalis muscle.
B. Symptom History
- Current symptoms started 3 months ago, not associated with any life event. The pain is constant, located in the right side of face and spreading to the frontal/temple area, graded 6 in intensity (NRS 0–10). Quality is dull, aching, sometimes burning, and remains for hours.
- The end of the day is the moment when the pain gets worse.
- Stress and concentration make the pain worse, while medication and relaxation are ameliorating factors.
- Awake and sleep bruxism are reported. No other parafunctional activities were reported.
C. Medical History
- No report of any medical problems or regular use of medication, other than a diagnosis of frequent tension-type headache made by a neurologist. Patient also reports the sporadic use of cyclobenzaprine (muscle relaxant), when her pain gets worse.
- No history of facial/head trauma or other accidents.
- No report of any aerobic physical activity.
D. Psychosocial History
- Patient has just got married, working in a private office and finishing writing her PhD thesis. Quality of sleep is good.
- Normal score for depression according to PHQ-9, but mild anxiety according to GAD-7. PHQ-15 showed moderate score for physical symptoms. Moderate level of stress according to PSS-10.
- No smoking or alcohol regular consumption reported.
E. Previous Consultations and Treatments
- Patient reported the first episode of facial pain about 6 years ago, accompanied by limited mouth opening, treated with NSAIDs, muscle relaxants, and physiotherapy. She reported mild relief after, but symptoms are recurrent, getting worse in the last 3 months.
F. Extraoral Status
Face
- No asymmetries, swelling, or other abnormality detected.
Mandibular active range of motion
- Jaw opening was straight. Maximum pain-free opening was 32 mm; maximum unassisted and assisted mouth opening was 40 mm with mild familiar pain on the right side of face, reproducing her chief complaint. Lateral and protrusive movements were within normal limits.
Temporomandibular joint
- No joint sound detected under manual inspection.
- Palpation of the both lateral and posterior aspects of the TMJs did not reveal any tenderness.
Masticatory muscle palpation
- Familiar pain on palpation was detected in the body of the right masseter. Pressure was then maintained, eliciting a referral pattern of pain to the frontal and temporal area, reproducing patient’s main complaint.
- No significant pain on cervical muscles was detected.
G. Intraoral Status
- Patient has a normal occlusion, wear facets were found in anterior dentition (Figure 3.9), along with bilateral indentation in the buccal mucosa (Figure 3.10). No other significant findings.

Figure 3.9 Wear facets on lower incisors.
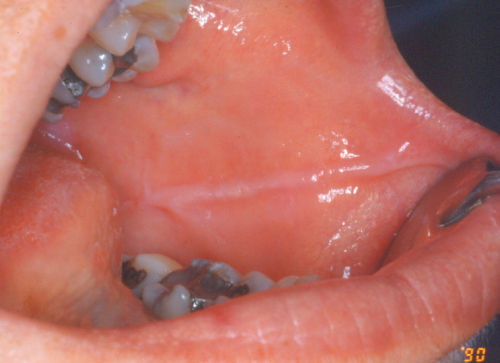
Figure 3.10 Indendation in the buccal mucosa.
H. Additional Examinations and Findings
- Vapor coolant spray was performed over the painful area followed by stretch of the masticatory muscles. Passive opening was increased with partial relief of the baseline pain (de Leeuw and Klasser, 2013).
I. Diagnosis/Diagnoses
DC/TMD
- Myofascial pain with referral.
ICHD-3
- Frequent tension-type headache.
Other
- Probable bruxism.
J. Case Assessment
- The case presented illustrates a typical manifestation of masticatory myofascial pain, a chronic muscular condition. An association of findings is probably responsible for the recurrence of patient’s symptoms. She is aware of sleep/awake bruxism/clenching, which, associated with indentations in the mucosa and dental wear facets, can be considered indicative of sleep/awake bruxism (Lobbezoo et al., 2013). No polysomnography was performed.
- Indeed, patient reported to be in a stressful phase of life, living in a new city, just married, and getting prepared to defend her PhD thesis. She also reported not to have free time to make any sort of aerobic physical activities.
- The reported stress, overload of masticatory muscles, and absence of physical activity are considered risk factors for muscle pain. Physical activity is considered an important method to stimulate pain modulation in chronic pain patients, by increasing the circulating endogenous opioids, and by decreasing pain transmission, among others (Mense and Gerwin, 2010).
- There is no strong scientific evidence for most of the modalities used to manage myofascial pain. Based on that, noninvasive and reversible modalities must be the first choice to manage such chronic conditions. In this case, reduction of muscles overload and increasing of modulatory system activity are fundamental management strategies.
K. Evidence-based Treatment Plan including Aims
- The implementation of a program to decrease the system overload has been demonstrated to be an efficient method to decrease TMD pain and to increase masticatory function (Conti et al., 2012). The self-regulation of the trigeminal system is able to reduce the amount of nociceptive stimuli to the brain, allowing the system to heal.
- Patients need to be carefully instructed about the importance of their participation in the management plan. Improving sleep quality, decreasing exposure to stressful situations, implementing relaxation techniques, decreasing caffeine intake, and avoiding masticatory/cervical muscles overfunction are important steps in this educational program.
- Patient was instructed to implement all these behavioral alterations and to practice home exercises, including biofeedback training to keep “lips together/teeth apart” while awake, decreasing daytime loading. Application of moist heat over the painful area for 15 min, two times a day, to decrease pain and assist muscle relaxation was also suggested. Patient was also encouraged to start practicing regular aerobic exercises and to avoid the use of over-the-counter medication for pain.
- Occlusal splints are one of the most used therapeutic modalities in the management of TMD of all sources, including myofascial pain. Muscle relaxation, decreasing overload to joints and muscles, reestablishment of an “ideal” occlusion, cognitive and sensorial impulses alterations, and placebo effect are frequently reported as probable mechanisms of action of these intraoral devices.
- Regardless of the mechanism involved, the use of occlusal splints has been supported by systematic reviews (Fricton et al., 2010). A precise occlusal design, the amount of increased vertical dimension of occlusion, and the ideal maxillomandibular position, however, seem not to play an important role in the efficacy of this modality.
- Among many types of devices, the stabilization splint is the most used. It is considered the safest, not leading to significant occlusal alterations, and it is relatively easy to fabricate.
- A flat, hard acrylic stabilization splint was delivered for use during sleep time (Figure 3.11). The splint design included bilateral simultaneous posterior contacts and anterior and canine guidance during excursive movements.

Figure 3.11 Occlusal stabilization appliance.
L. Prognosis and Discussion
- Myofascial pain is a relatively common diagnosis in the orofacial region. The phenomenon of referred pain, where the source of pain is different from the pain location, as described in this case, is frequently a common cause of confusion and results in inadequate management strategies. The management must always be directed to the source and not to the site of pain. A positive prognosis is highly dependent upon the patient’s adherence and collaboration to follow instructions on home care and exercises.
- The patient also has to be informed that the fundamental goal in the management of chronic pain conditions is to significantly decrease pain/dysfunction and to improve/increase mandibular function, and not necessarily “cure” the disease, considered as fluctuant, cyclic, and frequently associated with stressful life events (de Leeuw and Klasser, 2013).
Background Information
- Neuronal convergence and expansion of receptor fields, associated with peripheral and central sensitization, are probable mechanisms implicated in the phenomenon of referred pain, also known as heterotopic pain, where the source and site of pain are different.
- In case of pain in the head, it is always important to rule out the presence of a primary headache, which can be the patient’s main complaint and/or coexist with masticatory muscle pathologies (Costa et al., 2015).
- Although not required for this diagnosis, taut bands (i.e., contracture of muscle fibers) in the muscles may be present.
- TMJ disorders and pain, as well as systemic conditions (e.g., fibromyalgia), are frequently present in myofascial pain patients and should be considered when treatment is defined.
- The nociceptive information and transmission of the trigeminal system (responsible for masticatory pain sensation) is anatomically correlated with the upper cervical nerves (C1 to C3). Based on that, cervical myofascial pain can cause referred pain in trigeminal-related territories. In other words, one should be aware that cervical muscles are potential source of pain for face and head.
- Chronic and repetitive muscle contraction is frequently associated with myofascial pain. It has been suggested that some muscle fibers become overcontracted, leading to the pain sensation, associated with shortening of the muscle length (Mense and Gerwin, 2010).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


