A boy, aged 12 years 3 months, sought treatment for a complete unilateral Brodie bite. His maxillary dental arch was asymmetric, and his dentition was 10 mm wider than normal values for his age. The transverse discrepancy was his chief complaint because it caused a chewing dysfunction. We used a special slow maxillary contraction appliance, which contains a screw, connectors, and retainers, to contract the maxillary transverse asymmetric dental arch. This was followed by preadjusted fixed appliances to level the teeth and adjust the occlusion. A symmetric and functional Class I occlusion was achieved.
A Brodie bite is a type of posterior crossbite that causes interocclusal contact between the outer oblique surfaces of the maxillary lingual cusp and the mandibular buccal cusp. With a Brodie bite discrepancy, the maxillary dentition is wider or the mandibular dentition is narrower than normal, or both dentitions can be abnormal. A Brodie bite can be unilateral or bilateral and occurs in 1.0% to 1.5% of the population. The techniques for treating a complete unilateral or bilateral Brodie bite with transverse mandibular deficiency have been reported and include mandibular widening by distraction osteogenesis, mandibular transverse expansion by using cross-arch elastics, and expansion of the mandibular dental arch with a Schwarz appliance. A transverse skeletal deficiency (or narrow dentition) can be treated with mandibular widening (or dental arch expansion). However, can we treat a complete unilateral Brodie bite by constricting the maxillary dental arch if the maxillary asymmetric dentition is wider than normal?
In this case report, we address this question in our treatment of a teenaged patient with a complete unilateral Brodie bite on the right side. His maxillary asymmetric dentition was 10 mm wider than normal for children of his age. We successfully corrected his malocclusion with a slow maxillary contraction appliance followed by fixed appliance treatment.
Diagnosis and etiology
The patient was a boy, aged 12 years 3 months, with a complete unilateral Brodie bite. His chief complaint was chewing dysfunction. His soft-tissue profile was convex, with an open lip closure in resting status. His upper and lower lips were slightly thicker than normal ( Fig 1 ). His face was asymmetric. He had no signs or symptoms of a temporomandibular disorder.
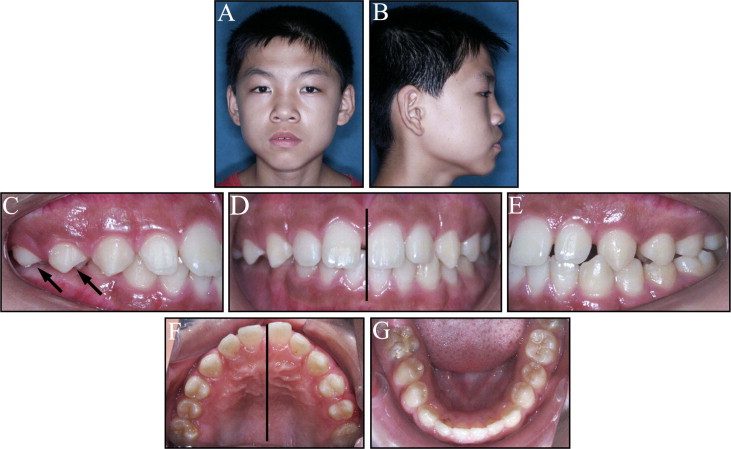
Intraorally, he had a dental Class III molar relationship and a Class I canine relationship on both sides ( Fig 1 ). His oral hygiene was excellent, and his periodontium was in good condition. The mesial margin of the maxillary left central incisor was coincident with the facial midline, but the right one deviated by 1.8 mm (a space between the maxillary incisors) to the right. The mandibular dental midline was the same as the facial midline in centric occlusion. His right lateral occlusion was a complete unilateral Brodie bite with an asymmetric maxillary dentition.
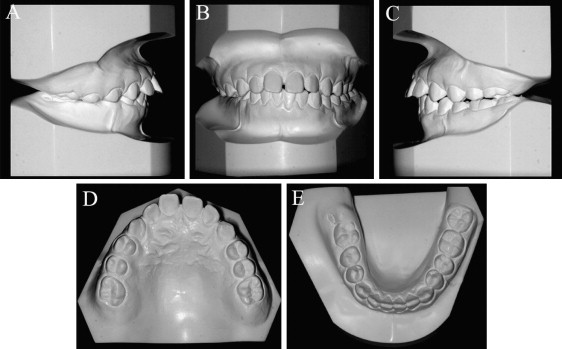
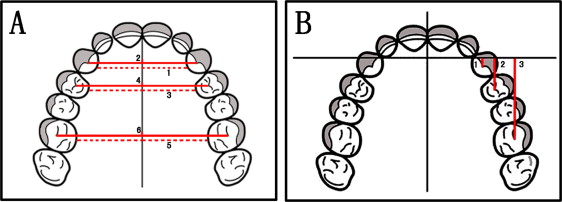
Analysis of the dental casts showed a dental Class III relationship ( Fig 2 ). The spaces between the maxillary right first molar and left first premolar were 15 mm. A wide, severe maxillary transverse process was a problem. The maxillary first molar’s cross-arch width (44.40 mm) was greater than normal (34.69 mm) in children of his age. The maxillary dental arch was asymmetric, with the right side larger than the left. The mandibular first molar’s cross-arch width (33.91 mm) was nearly normal (32.50 mm). The mandibular right second premolars were slightly inclined lingually. Transverse and sagittal measurements are shown in Figure 3 and Table I .
| Pretreatment | After SMC | Posttreatment | Retention | T1-T0 | T2-T1 | T3-T0 | T3-T2 | |
|---|---|---|---|---|---|---|---|---|
| T0 (12 y 3 mo) | T1 (12 y 10 mo) | T2 (14 y 8 mo) | T3 (17 y 9 mo) | |||||
| Transverse measurements (mm) | ||||||||
| Maxillary canine cross-arch width | 30.36 | 26.08 | 28.35 | 27.86 | −4.28 | 2.27 | −2.50 | −0.49 |
| Maxillary intercanine width | 39.35 | 34.14 | 37.23 | 37.20 | −5.21 | 3.09 | −2.15 | −0.03 |
| Left | 19.15 | 17.51 | 18.61 | 18.60 | −1.64 | 1.10 | −0.55 | −0.01 |
| Right | 20.20 | 16.63 | 18.62 | 18.60 | −3.57 | 1.99 | −1.60 | −0.02 |
| Maxillary first premolar cross-arch width | 36.15 | 30.40 | 32.21 | 32.32 | −5.75 | 1.81 | −3.83 | 0.11 |
| Maxillary interfirst premolar width | 45.06 | 38.90 | 40.75 | 41.94 | −6.16 | 1.85 | −3.12 | 1.19 |
| Left | 21.78 | 20.06 | 20.37 | 20.96 | −1.72 | 0.31 | −0.82 | 0.59 |
| Right | 23.28 | 18.84 | 20.38 | 20.98 | −4.44 | 1.54 | −2.30 | 0.60 |
| Maxillary first molar cross-arch width | 44.40 | 39.13 | 39.62 | 39.94 | −5.27 | 0.49 | −4.46 | 0.32 |
| Maxillary interfirst molar width | 56.09 | 50.33 | 50.86 | 51.78 | −5.76 | 0.53 | −4.31 | 0.92 |
| Left | 27.34 | 25.43 | 25.56 | 25.95 | −1.91 | 0.13 | −1.39 | 0.39 |
| Right | 28.75 | 24.90 | 25.30 | 25.83 | −3.85 | 0.40 | −2.92 | 0.53 |
| Maxillary cross-arch alveolar process width | 60.17 | 56.86 | 60.32 | 63.18 | −3.31 | 3.46 | 3.01 | 2.86 |
| Mandibular interfirst molar width | 33.91 | 35.42 | 35.48 | 36.55 | 1.51 | 0.06 | 2.64 | 1.07 |
| Sagittal measurements (mm) | ||||||||
| Canine distance | ||||||||
| Left | 2.87 | 2.58 | −1.28 | −0.77 | −0.29 | −3.86 | −3.64 | 0.51 |
| Right | 2.86 | 2.13 | −1.10 | −0.69 | −0.73 | −3.23 | −3.55 | 0.41 |
| First premolar distance | ||||||||
| Left | 12.34 | 12.05 | 7.39 | 8.02 | −0.29 | −4.65 | −4.32 | 0.63 |
| Right | 11.44 | 10.55 | 7.61 | 8.16 | −0.89 | −2.94 | −3.28 | 0.55 |
| First molar distance | ||||||||
| Left | 27.31 | 27.01 | 22.38 | 23.01 | −0.30 | −4.63 | −4.30 | 0.63 |
| Right | 30.22 | 27.95 | 23.3 | 23.98 | −2.27 | −4.65 | −6.24 | 0.68 |
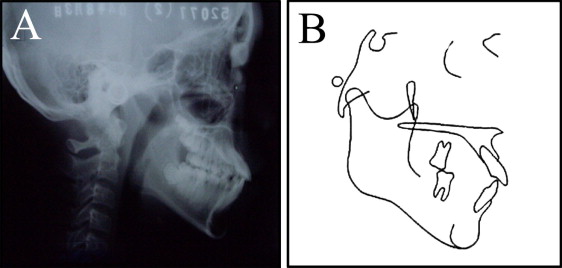
The cephalometric analysis showed a skeletal Class I relationship, with a slight downward and backward rotation of the mandible ( Fig 4 ; Table II ). The maxillary incisors appeared to be severely tipped labially. A pretreatment panoramic radiograph showed a healthy periodontium, with endodontic treatment of the mandibular right first molar.
| Measurement | Mean | SD | Pretreatment | Posttreatment | Retention | T1-T0 | T2-T1 | T2-T0 |
|---|---|---|---|---|---|---|---|---|
| T0 (12 y 3 mo) | T1 (14 y 8 mo) | T2 (17 y 9 mo) | ||||||
| Skeletal (°) | ||||||||
| SNA | 80.8 | 4.0 | 81.2 | 82.0 | 81.3 | 0.8 | −0.7 | 0.1 |
| SNB | 80.1 | 3.9 | 79.4 | 78.8 | 79.2 | −0.6 | 0.4 | −0.2 |
| ANB | 2.7 | 2.0 | 1.8 | 3.4 | 2.1 | 1.6 | −1.3 | 0.3 |
| SN-MeGo | 32.5 | 5.2 | 35.5 | 34.1 | 34.6 | −1.4 | 0.5 | −0.9 |
| SN-Gn | 65.8 | 4.2 | 67.0 | 66.4 | 66.9 | −0.6 | 0.5 | −0.1 |
| Dental (°) | ||||||||
| U1 to SN | 105.7 | 6.3 | 119.3 | 109.5 | 113.6 | −9.8 | 4.1 | −5.7 |
| L1 to MeGo | 96.9 | 6.0 | 94.3 | 91.1 | 91.7 | −3.2 | 0.6 | −2.6 |
| U1 to L1 | 124.2 | 8.2 | 110.0 | 124.0 | 120.1 | 14 | −3.9 | 10.1 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


