In this article, we report the orthodontic treatment of a boy (age 12 years 9 months) who had a midface deficiency, a concave facial profile with maxillary retrusion, a complete crossbite (anterior and posterior), and the maxillary right canine retained in the alveolus. Rapid maxillary expansion was performed followed by complete orthodontic treatment with fixed appliances combined with Class III elastics and anterior vertical elastics. Time was allowed to elapse until growth was virtually over before removing the fixed appliances (at age 18 years 4 months), and no retainer of any type was used. As a result of treatment, significant improvement was noted in his facial appearance, with a proper maxillomandibular relationship, total correction of the maxillary atresia, and satisfactory overjet and overbite. The results remained stable at the 4-year follow-up. Therefore, it can be argued that the use of Class III elastics combined with rapid maxillary expansion has a beneficial effect in the treatment of transverse and sagittal maxillary deficiency in growing patients. Excellence in how the treatment was finished and discontinuation of treatment and control in the final stages of growth contributed to the stability of the final results.
Highlights
- •
Transverse deficiencies during growth are best solved with rapid maxillary expansion (RME).
- •
Forces generated by Class III elastics are similar to forces generated by reverse traction or chincup.
- •
Cooperation with class III elastics is better and longer than with reverse traction or chincup.
- •
Time to stop class III treatment should be when growth ends, increasing treatment time.
- •
Correction of anterior crossbites does not require any kind of retention for stable results.
Despite a lower prevalence of Angle Class III malocclusion compared with Class I and Class II in the population, treating the former poses a daunting challenge to the orthodontist, especially in patients with skeletal involvement. The therapeutic options available for correction of Class III malocclusion in growing patients include the use of a chincup, expansion and reverse pull of the maxilla, functional orthopedic appliances, headgear for the mandibular arch, and Class III elastics.
Inducing a clockwise rotation of the mandible to correct a Class III relationship and improve the facial profile by moving the chin downward and backward is a rather common strategy today. There are, however, 2 caveats to this approach. First, it should not be used in patients with a high mandibular plane angle, increased lower anterior face height, and open bite. These features are common in skeletal Class III malocclusions. Second, the stability of treated patients is more intimately related to therapeutic approaches that achieve an adequate overbite without producing mandibular clockwise rotation.
This case report describes the orthodontic treatment performed on a boy with maxillary sagittal and transverse deficiencies between the ages of 12 and 18 years. Rapid maxillary expansion (RME) was used, followed by fixed orthodontic appliances with Class III and vertical elastics. The results remained stable after 4 years without any kind of retention.
Diagnosis and etiology
A boy, aged 12 years 9 months, came to the Department of Orthodontics of Fluminense Federal University in Brazil accompanied by his mother and seeking orthodontic care. His major complaints were retrusion of the upper lip, lack of maxillary teeth, dental misalignment, and compromised phonation. The medical history showed that the patient was taking carbamazepine (200 mg) to prevent seizures; this did not contraindicate orthodontic therapy.
The extraoral examination disclosed a slightly concave profile with deficiency in the midface and retrusion of the upper lip relative to the lower lip. In the front view, there were symmetry, passive lip seal, normal smile line, and deviation of the maxillary teeth to the right ( Fig 1 ). There was some deviation in the mandibular closing pattern and clicks in the temporomandibular joints. Swallowing, phonation, and tongue position were also altered. In addition, the patient displayed oral breathing, although his nose breathing was intact.

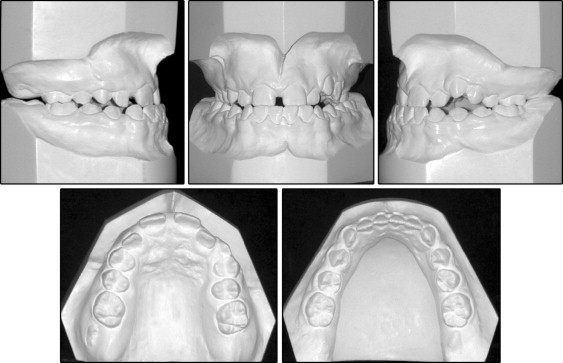
Intraorally, the maxillary arch was totally circumscribed by the mandibular arch, which characterized a complete crossbite (both anterior and posterior). The lack of space in the maxilla amounted to 11.6 mm, with a lack of space also for both canines. The maxillary right canine was totally retained. The mandibular arch, in turn, showed a positive discrepancy of 3 mm. Overjet was −1 mm (negative), and the right incisors were shifted to the right, with a related diastema. The molar relationship was Class I, and there was an open bite in the region of the left canines ( Fig 2 ).
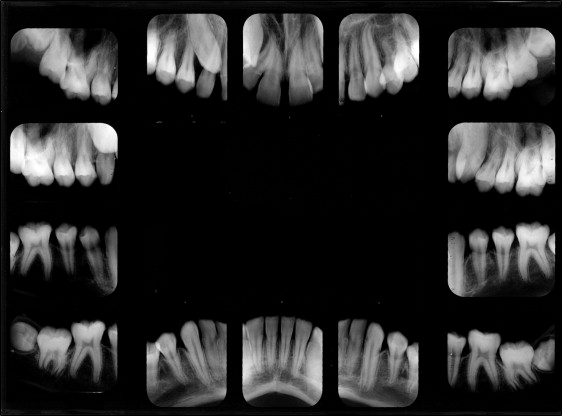
The radiographic examination ( Figs 3 and 4 ) showed the presence of all teeth, including the third molars in the final stages of crown formation, with the maxillary third molars showing some distal tip and the mandibular third molars some mesial tip. The maxillary right canine could be visualized and had a slight mesial tip. It was impacted between the roots of the lateral incisor and the right first premolar. No changes were noted in the bone or the periodontal and periapical aspects.

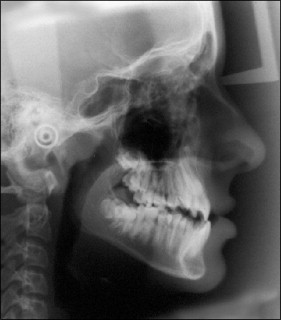
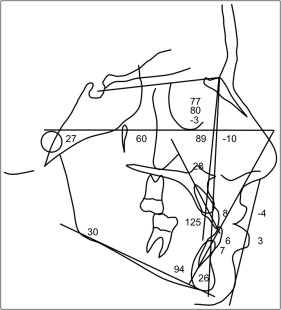
The cephalometric analysis ( Figs 5 and 6 ; Table ) disclosed maxillary retrusion relative to the cranial base (SNA, 77°; SNB, 80°; ANB, −3°), and the relationship between the basal bones as measured by AO-BO (Wits appraisal) was −8 mm. There was a favorable vertical relationship (SN. GoGn, 30°; FMA, 27°), a concave skeletal profile (facial convexity, −10°), and an unbalanced lip relationship (S-LS, −4 mm; S-LI, +3 mm). The maxillary incisors protruded labially (1-NA, 8 mm; 1.NA, 28°), and the mandibular incisors had a moderate labial inclination (1-NB, 6 mm; 1.NB, 26°; IMPA, 94°) without signs of Class III compensation. The patient was going through a stage of active growth; therefore, the intermaxillary sagittal relationship was likely to worsen without intervention.
| Measurement | Normal | Pretreatment | Posttreatment | Follow-up |
|---|---|---|---|---|
| Age | 12 y 9 mo | 18 y 4 mo | 22 y 7 mo | |
| Skeletal pattern | ||||
| SNA (°) | 82 | 77 | 80 | 80 |
| SNB (°) | 80 | 80 | 80 | 80 |
| ANB (°) | 2 | −3 | 0 | 0 |
| Facial convexity (°) | 0 | −10 | −4 | −4 |
| Y-axis (°) | 59 | 60 | 62 | 63 |
| Facial angle (°) | 87 | 89 | 90 | 91 |
| SN.GoGn (°) | 32 | 30 | 30 | 31 |
| AO-BO (mm) | −1 | −8 | −5 | −6 |
| Dental pattern | ||||
| IMPA (°) | 90 | 94 | 93 | 92 |
| 1.NA (°) | 22 | 28 | 30 | 29 |
| 1-NA (mm) | 4 | 8 | 7 | 7 |
| 1.NB (°) | 25 | 26 | 24 | 23 |
| 1-NB (mm) | 4 | 6 | 5 | 5 |
| 1.1 (°) | 130 | 125 | 127 | 129 |
| Profile | ||||
| Upper lip, S line (mm) | 0 | −4 | −2 | −1 |
| Lower lip, S line (mm) | 0 | 3 | 1 | 1 |
Treatment objectives
The treatment objectives were to (1) improve the facial appearance by protruding the midface (maxilla) anteriorly and thus correct the unbalanced relationship between the upper and lower lips; (2) correct the posterior and anterior crossbites; (3) improve the dental relationships, especially of the molars and incisors, to achieve proper occlusion with appropriate overjet and overbite; (4) make space for the maxillary canines; (5) achieve a mutually protected functional occlusion with stable and simultaneous occlusal contacts of all teeth in central relationship and eccentric contacts guided by the anterior teeth; (6) eliminate the signs of temporomandibular joint dysfunction; and (7) ensure that the patient breathed mostly through the nose.
Treatment objectives
The treatment objectives were to (1) improve the facial appearance by protruding the midface (maxilla) anteriorly and thus correct the unbalanced relationship between the upper and lower lips; (2) correct the posterior and anterior crossbites; (3) improve the dental relationships, especially of the molars and incisors, to achieve proper occlusion with appropriate overjet and overbite; (4) make space for the maxillary canines; (5) achieve a mutually protected functional occlusion with stable and simultaneous occlusal contacts of all teeth in central relationship and eccentric contacts guided by the anterior teeth; (6) eliminate the signs of temporomandibular joint dysfunction; and (7) ensure that the patient breathed mostly through the nose.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


