Introduction
Identification of the dental arch form of the orthodontic patient is a key aspect for achieving a stable, functional, and esthetic dentition. Failure to customize preformed archwires with the patient’s arch form might increase the probability of relapse and lead to an unnatural smile. The primary objective of this study was to identify the arch forms of Israeli subjects with dental normocclusion and malocclusions. The secondary objective was to clarify the morphologic differences between Israeli and North American white subjects with various malocclusions.
Methods
The sample included 134 Israeli (40 Class I, 61 Class II, and 33 Class III) and 160 North American (60 Class I, 50 Class II, and 50 Class III) subjects. The most facial portion of 13 proximal contact areas was digitized from photocopied images of the mandibular dental arches. Clinical bracket points were calculated for each tooth based on mandibular tooth thickness data. Four linear and 2 proportional measurements were made. The dental arches were classified as square, ovoid, and tapered forms to determine and compare the frequency distributions between the 2 ethnic groups.
Results
The most frequent mandibular arch form of the Israeli group was found to be ovoid as opposed to tapered in the North American white group. The white population had statistically significant decreased arch widths and increased arch depths compared with the Israeli population. The analysis of the Israeli sample indicated that, as the malocclusion shifts from Class III through Class I to Class II, the weight of the arch form tends to shift from square and ovoid to ovoid and tapered.
Conclusions
Our results suggest that, when treating Israeli patients, one should expect to use the preformed ovoid arch form orthodontic wires in a significant percentage of patients.
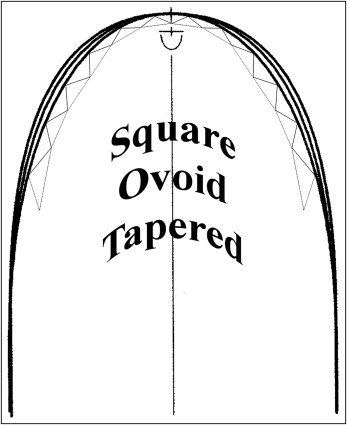
The use of preformed archwires is widespread in orthodontics. Well-aligned dental arches are roughly categorized as square, ovoid, and tapered ( Fig 1 ). Identification of the dental arch form of the orthodontic patient is an important parameter in achieving a stable, functional, and esthetic dentition. Failure to customize preformed archwires with the patient’s arch form might increase the probability of relapse and lead to an unnatural smile. Some researchers have attempted to identify an arch form unique to a certain ethnic group, but most studies compare average clinical arch forms from normal untreated subjects.
Over the years, many geometric forms and mathematical functions have been proposed as models of the dental arch. However, 1 arch form will not provide the best solution for the entire orthodontic population. Although modern orthodontists frequently use preformed flexible and rigid archwires, we believe that arch-form analysis, which is based on clinical bracket points, is of the highest clinical relevance.
Whereas the dolichocephalic head form is the most common among North American whites, the Israeli population originates from heterogeneous ethnic backgrounds and might well differ from the white population (Jewish). Israeli Jews have several distinct ethnic divisions—Ashkenazim, Mizrahim, and Sephardim; most are primarily the result of geographic branching from an original Israelite population and subsequent independent evolutions.
Today, manifestation of these ethnic divisions can be observed mainly in the Jewish cultural expressions of each community, as well as degrees and sources of genetic admixtures. Yet, now there is growing evidence that the modern Jewish Israeli population differs from the older Jewish population and has the characteristics of mixed ethnicity. These conclusions were based on the comparison of head forms of conserved Semite populations in the Middle East. Studies showed that people known to be of Semitic origin are dolichocephalic, whereas modern Jews are mesocephalic or even extremely brachycephalic. This refers mainly to sabras (Israeli-born), who are mostly second- or third-generation Israelis. Although there is a well-studied correlation between racial head forms and arch forms (arch width and depth parameters), one should consider both arch form parameters and dental malocclusion classifications before the final determination of a patient’s optimal dental arch form.
The primary objective of this study was to identify the arch form distribution in an Israeli population of subjects with normocclusion and dental malocclusions. The secondary objective was to clarify the morphologic differences between Israeli and North American white populations with various malocclusions by measuring their dental arch dimensions.
Material and methods
Arch form shape was determined according to the method described by Nojima et al. Briefly, the most facial portion of 13 proximal contact areas was digitized from photocopied images of the mandibular dental arches. Clinical bracket points were calculated for each tooth based on mandibular tooth thickness data. Four linear and 2 proportional measurements were made. The dental arches were classified into square, ovoid, and tapered forms to determine and compare the frequency distributions between the 2 ethnic groups. For the statistical analysis, categorical variables, frequencies, percentages, and distributions were calculated. For continuous variables, ranges, means, and standard deviations were calculated. Distributions of categorical variables were compared and analyzed with the chi-square-test. The results of the continuous variables were compared by analysis of variance (ANOVA) (for 3 subgroups) or by 2-sample t tests for differences in means (for 2 subgroups).
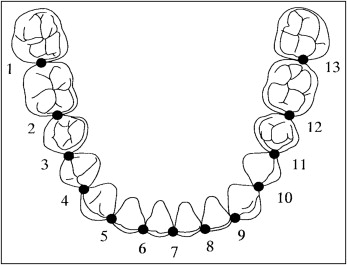
This study was based on 2 sample groups of Israeli and North American white subjects. The Israeli group consisted of the pretreatment mandibular dental models from 40 Class I, 61 Class II, and 33 Class III sabra patients obtained from the Department of Orthodontics, Hebrew University, Hadassah School of Dental Medicine, in Jerusalem. The North American white group consisted of models of 60 Class I, 50 Class II, and 50 Class III patients from the University of Southern California, Department of Orthodontics, Los Angeles, and a private practice in San Diego, Calif ( Table I ). All patients met the following inclusion criteria: (1) Angle dental Class I, Class II, or Class III malocclusion, (2) permanent dentition with normal tooth size and shape, (3) 3-mm or less arch-length discrepancy, and (4) no restorations extending to contact areas, cusp tips, or incisal edges. The occlusal surfaces of the mandibular models were photocopied, with a ruler included for magnification correction. The photocopied images were placed on a digitizer, and the most facial portions of 13 proximal contact areas around the arch were digitized ( Fig 2 ). These points were used to estimate corresponding bracket slot locations (clinical bracket point) for each tooth. The proximal contact between the 2 central incisors was used as the origin of the x-y coordinates. The original x-y coordinates on the digitizer were corrected for magnification and adjusted to establish a new x = y = coordinate so that the mean inclination of straight lines connecting the right and left contact points between the first and second premolars and those between the second premolars and the first molar became parallel to the original x-axis.
| White (n = 160) |
Israeli (n = 134) |
P † | |
|---|---|---|---|
| Sex, % (n) | |||
| Total | |||
| Male | 47.5 (76) | 38.1 (51) | 0.104 |
| Female | 52.5 (84) | 61.9 (83) | |
| Class I | |||
| Male | 38.3 (23) | 42.5 (17) | 0.677 |
| Female | 61.7 (37) | 57.5 (23) | |
| Class II | |||
| Male | 52.0 (26) | 31.1 (19) | 0.026 ∗ |
| Female | 48.0 (24) | 68.9 (42) | |
| Class III | |||
| Male | 54.0 (27) | 45.5 (15) | 0.446 |
| Female | 46.0 (23) | 54.5 (18) | |
| Age (y), median (range) † | |||
| Total | 13.7 (8.5-35.5) | 18.0 (9-44) | |
| Class I | 13.6 (11.3-36.0) | 18.0 (14-32) | |
| Class II | 13.6 (10.4-35.5) | 17.0 (10-44) | |
| Class III | 13.8 (8.5-30.6) | 18.0 (9-44) | |
The perpendicular to a line connecting the mesial and distal contact points of each tooth on the coordinate was drawn from the midpoint of the mesiodistal line for the incisors, canines, and premolars and from the mesial third of the line for the molars. The perpendicular was extended labially or buccally to locate a clinical bracket point for each tooth, according to the mandibular tooth thickness data of Andrews.
The following 4 linear and 2 proportional measurements were made ( Fig 3 ): (1) intercanine width, the distance between the canine clinical bracket points; (2) intermolar width, the distance between the first molar clinical bracket points; (3) canine depth, the shortest distance from a line connecting the canine clinical bracket points to the origin between the central incisors; (4) molar depth, the shortest distance from a line connecting the first molar clinical bracket points to the origin between the central incisors; (5) canine width-depth (WD) ratio, the ratio of intercanine width and canine depth; (6) molar WD ratio, the ratio of intermolar width and molar depth.
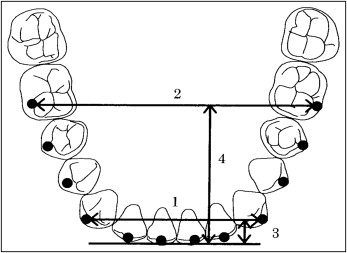
In addition, 12 clinical bracket points per patient were printed at full size to select from square, ovoid, and tapered arch forms (OrthoForm, 3M Unitek, Monrovia, Calif) the arch form that best fit the 8 clinical bracket points from first premolar to first premolar ( Fig 3 ).
Statistical analysis
The measurements for the statistical analysis and evaluations were taken from 3 types of arch form (tapered, square, ovoid) at the 3 Angle classifications (Class I, Class II, Class III). For the categorical variables, frequencies, percentages, and distribution were calculated. For the continuous variables, ranges, means, and standard deviations were calculated. Distributions of categorical variables were compared and analyzed by the chi-square-test. The results of the continuous variables were compared by analysis of variance (ANOVA) (for 3 subgroups) or by 2-sample t test for differences in means (for 2 subgroups). All analyses were tested at the significance level of 0.05. Measurement errors were assessed by statistically analyzing the difference between duplicate measurements taken at least 2 weeks apart on 24 casts selected at random. The measurement errors were generally small (less than 5% of the measured mean value) and within acceptable limits.
Results
Our results indicated that, in the entire sample group, the Israeli arch is wider and shows significantly lower values of both canine and molar depths, compared with the North American sample. This results in significantly higher canine and molar WD ratios ( Table II ).
| Total (n = 294) | |||
|---|---|---|---|
| Variable | White (n = 160) mean (SD) |
Israeli (n = 134) mean (SD) |
P ‡ |
| Intercanine width (mm) | 29.1 (1.52) | 29.52 (1.52) | 0.019 ∗ |
| Intermolar width (mm) | 49.5 (2.53) | 50.12 (2.55) | 0.038 ∗ |
| Canine depth (mm) | 6.22 (1.26) | 4.52 (1.08) | 0.0001 † |
| Molar depth (mm) | 27.0 (2.15) | 24.85 (1.88) | 0.0001 † |
| Canine WD ratio | 4.8 (1.01) | 6.90 (1.84) | 0.0001 † |
| Molar WD ratio | 1.8 (0.13) | 2.04 (0.17) | 0.0001 † |
When we evaluated all Angle malocclusions, the results showed that the Israeli sample had significantly lower values for canine and molar depths and, as a direct result, higher values for both canine and molar WD ratio compared with the white American sample. Class II malocclusion values also showed a significant difference in intermolar width compared with the molar widths of the Class I and Class III malocclusions ( Table III ).
| Class I (n = 100) | Class II (n = 111) | Class III (n = 83) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | White (n = 60) mean (SD) | Israeli (n = 40) mean (SD) | P ‡ | White (n = 50) mean (SD) | Israeli (n = 61) mean (SD) | P ‡ | White (n = 50) mean (SD) | Israeli (n = 33) mean (SD) | P ‡ |
| Intercanine width (mm) | 29.0 (1.63) | 29.37 (1.53) | 0.257 (NS) | 28.9 (1.48) | 29.52 (1.56) | 0.035 ∗ | 29.3 (1.63) | 29.72 (1.48) | 0.237 NS |
| Intermolar width (mm) | 49.4 (2.40) | 49.71 (2.64) | 0.545 (NS) | 48.6 (2.47) | 50.20 (2.40) | 0.0008 † | 50.8 (2.62) | 50.48 (2.74) | 0.545 NS |
| Canine depth (mm) | 6.3 (1.08) | 4.46 (1.09) | 0.0001 † | 6.8 (1.34) | 4.80 (1.04) | 0.0001 † | 5.6 (1.13) | 4.18 (1.03) | 0.0001 † |
| Molar depth (mm) | 26.7 (1.94) | 24.66 (1.88) | 0.0001 † | 27.3 (2.12) | 25.06 (1.64) | 0.0001 † | 26.8 (2.12) | 24.30 (2.24) | 0.0001 † |
| Canine WD ratio | 4.7 (0.93) | 6.96 (1.68) | 0.0001 † | 4.4 (0.99) | 6.52 (1.91) | 0.0001 † | 5.4 (1.06) | 7.51 (1.75) | 0.0001 † |
| Molar WD ratio | 1.85 (0.14) | 2.03 (0.18) | 0.0001 † | 1.79 (0.14) | 2.01 (0.14) | 0.0001 † | 1.91 (0.21) | 2.09 (0.19) | 0.0002 † |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


