9Clinical Case Presentations
9.1.1Iatrogenic Complications Managed by Replacing Prosthetic Components: Non-surgical Approach
B. Schmid
A male patient had lost teeth 11 and 22 as a result of a bicycle accident at age 14. In his adolescent years, a removable prosthesis had replaced the missing teeth. At age 21, the patient was referred by his dentist to the university clinic for treatment of the missing teeth 11 and 22 with implants. He was in good health and a non-smoker. The absence of teeth 11 and 22 over many years had led to significant atrophy of the alveolar ridge, particularly at site 11. As a first step, the alveolar ridge was augmented using a block graft to replace the lost bone. A Straumann SP implant (diameter 4.1 mm, length 12 mm; Institut Straumann AG, Basel, Switzerland) and a Straumann Narrow Neck implant (length 10 mm) were inserted in the correct location and axial position at sites 11 and 22, respectively, six months later. After three months of healing and subsequent reentry, the patient returned to the referring dentist to receive the prosthetic restoration. The patient was seen again six months after the restoration had been placed. The frontal view showed a high smile line, an irregular gingival profile, and a bluish-gray tinge to implant crowns 11 and 22 compared to the natural dentition (Fig 1).


Under magnification, a slightly shorter incisal edge of implant crown 11 as well as pronounced reddening accompanied by fistula formation at the buccal aspect of implant 11 (Fig 2) was observed. Crowns 11 and 22 had been cemented. The radiographs showed a distinct gap, particularly at implant 11, between the implant shoulder and the edge of the crown (Figs 3a–b).
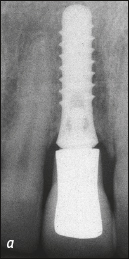
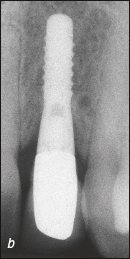
Figs 3a-b Implants 11 und 22 at baseline. (a) Distinct gap between the implant and the crown due to a cementing error at implant 11. (b) At implant 22, only a small cementing error is seen.
As the crowns had been cemented, strong compression resulted in cement residue being deposited in the soft tissue, which was responsible for the inflammation (mucositis) around the implant. If cement residue is present, associated bone loss (peri-implantitis) is frequently the long-term result.
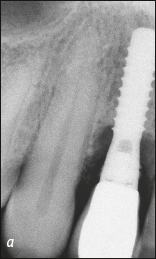
Figures 3c–d show a case six years after cementation of an implant-supported anterior crown with bone loss due to peri-implantitis as well as cement residue around the Narrow Neck implant.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


