A 23-year-old woman with a skeletal Class III relationship, a normal vertical jaw relationship, and missing maxillary lateral incisors was treated with bidimensional fixed edgewise appliance therapy combined with orthognathic surgery. A functional and esthetic occlusion in an improved facial profile was established at the end of the surgical and orthodontic treatment. Pretreatment, posttreatment, and long-term follow-up records for the patient are presented.
Class III malocclusion can involve only the dentition, or it might be complicated by a poor relationship between the maxilla and the mandible. In the former situation, the mandibular first molar is positioned half a cusp toward the midline with respect to the maxillary molar, whereas the latter type also involves a poor relationship between the maxilla and the mandible in the sagittal plane, caused by maxillary retrusion or mandibular protrusion. In addition, a retruded maxilla is frequently accompanied by skeletal constriction in the transverse plane. The majority of Class III patients have both dentoalveolar and skeletal components.
Various factors are implicated in the etiology of a Class III malocclusion: heredity (eg, race), environmental factors (eg, functional anterior deviation of the mandible or mouth breathing, which can be a positive stimulus for mandibular growth), and several pathologies (eg, pituitary tumors responsible for acromegaly).
The incidence of this type of malocclusion in white populations varies between 1% and 5%; in Asian populations, it reaches an upper range between 9% and 19%; and in Latin populations, it is about 5%.
Early treatment of Class III malocclusion reduces the necessity of a second phase of treatment. Several studies have reported that Class III skeletal discrepancies worsen with age. Thus, the difficulty in treating preadolescent patients successfully increases over time. Nonetheless, most patients with severe skeletal Class III malocclusion are candidates for orthognathic surgery in adulthood, the only means of obtaining functional occlusion and an esthetically pleasing profile. Moreover, many adults presenting for comprehensive orthodontic therapy have additional dental and periodontal problems that require multidisciplinary treatment approaches.
The aim of this case report was therefore to present the interdisciplinary treatment of an adult patient with a Class III malocclusion complicated by missing maxillary lateral incisors.
Diagnosis and etiology
A 23-year-old woman reported with the principal complaint of unsatisfactory esthetic appearance of her teeth. Her medical history showed no contraindication to orthodontic therapy, and no history of trauma or serious illness. Facial photographs showed maxillary retrusion and severe mandibular protrusion with an unesthetic smile ( Fig 1 ). Intraoral examination of the maxillary dental arch showed a transverse skeletal constriction, a diastema between the central incisors, and congenital absence of the permanent lateral incisors.

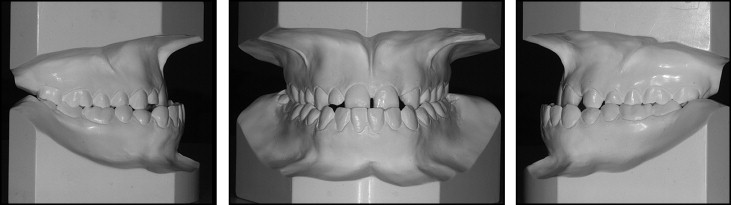
In the mandibular arch, on the other hand, mild incisor crowding, and anterior and bilateral crossbite with negative overjet (−6.5 mm) were evident. The tooth discoloration was probably due to tetracycline administration during dental development. Class III molar and canine relationships were observed on both the right and left sides. The mandible deviated toward the right. The maxillary left lateral incisor edentulous space had been partially closed by migration of the adjacent teeth ( Fig 2 ).
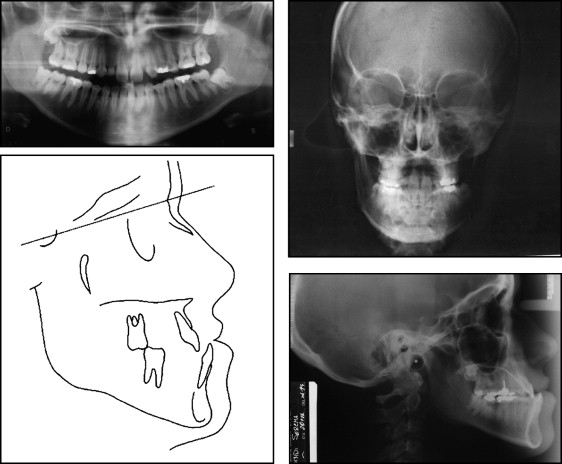
Evaluation of the panoramic radiograph confirmed that the maxillary lateral incisors were missing and showed the impacted maxillary and mandibular third molars ( Fig 3 ). Cephalometric analysis showed a skeletal Class III relationship, normal vertical jaw proportions (SNA-SNP/Go-Gn, 23°), and inclined mandibular incisors (lower incisor^GoGn, 84°).
Treatment alternatives
Three treatment options were proposed to the patient. The first would involve orthodontic treatment of the maxillary and mandibular arches, reopening of the maxillary lateral incisor space, and surgical treatment to correct the vertical and sagittal skeletal discrepancies. This option would also include replacing the missing maxillary lateral incisors with 2 dental implants. Although this solution would produce Class I molar and canine relationships on both sides, the gingival contour and margin levels would be critical and difficult to control in the long term.
Another option consisted of closing the spaces left by the congenitally missing teeth before bimaxillary surgery. This choice would also require restoration of the maxillary canines to resemble lateral incisors and the first premolars to simulate canines.
The third choice was nonsurgical orthodontic treatment. This option would involve extraction of the mandibular first premolars and replacement of the missing maxillary lateral incisors with 2 dental implants. The premolar extractions and opening of the lateral incisor spaces would permit resolution of the anterior crossbite and achieve an occlusal compromise. However, neither facial esthetics, skeletal asymmetry, nor the transverse discrepancy would be improved.
After consultation, the patient chose the second option, and her treatment course and outcome are detailed below.
Treatment plan
Levelling and alignment of both arches and closure of the lateral incisor spaces were the first steps. Then LeFort I surgery would be used to correct the vertical and transverse skeletal discrepancies and to assist in sagittal coordination of the mandible. Finally, bilateral sagittal split ramus osteotomy would be used to correct the asymmetry, prognathism, sagittal maxillomandibular relationship, and dental malocclusion. The final steps would be occlusal finishing and restorative rehabilitation of the maxiillary canines and first premolars to substitute as lateral incisors and achieve adequate occlusal and esthetic results.
Treatment progress
The mandibular third permanent molars and maxillary right deciduous lateral incisor were extracted. Although a bidimensional appliance was used initially, the maxillary second molars were not bonded, and the maxillary canines were fitted with conventional fixed appliances (0.022 × 0.028 in) to facilitate sliding mechanics of the maxillary central incisors.
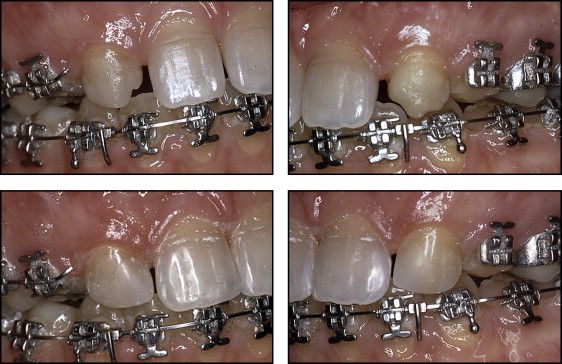
Leveling and alignment were begun with a 0.014-in nickel-titanium archwire and completed with a 0.016 × 0.022-in stainless steel wire. Space closure was achieved by using 0.018 × 0.022-in stainless steel archwires, selected to maintain incisor torque control (0.018 × 0.025-in slot) and reduce friction on the canines, premolars, and molars during incisor retraction (brackets, 0.022 × 0.028 in) ( Fig 4 ).
After bimaxillary surgery, esthetic recontouring of the maxillary canines was accomplished by using a combination of grinding and composite resin buildups ( Fig 5 ). In addition, the maxillary canines, which had been reshaped as lateral incisors, were fitted with new 0.018 × 0.025-in brackets (bidimensional prescription) to provide precise control of torque and tipping, and the mandibular second molars were banded. After rebracketing of the maxillary canines (lateral incisors), a 0.016 × 0.022-in Quad-Cat (GAC International, Bohemia, NY) archwire was placed.