Key points
- •
Chromosomal aneuploidies are caused by nondisjunction of chromosomes in meiosis or mitosis.
- •
Down syndrome is caused by trisomy of chromosome 21.
- •
Klinefelter and Turner syndromes are sex chromosome aneuploidies, with an extra X chromosome in the former and a missing X in the latter.
- •
Mosaicism is found in Down syndrome, Klinefelter syndrome, and Turner syndrome.
- •
The risk of Down syndrome and Klinefelter syndrome increases with maternal age, but this phenomenon is not observed for Turner syndrome.
- •
The main features of Down syndrome are cognitive impairment, hypotonia, and characteristic facial features.
- •
The 2 main features of Klinefelter syndrome are hypergonadotropic hypogonadism and small testicular volume, although most individuals with Klinefelter syndrome remain undiagnosed.
- •
The 2 main features of Turner syndrome are growth retardation, resulting in short stature throughout life, and infertility in later years.
Down syndrome
Genetics
Down syndrome is the most frequently observed chromosomal aneuploidy caused by trisomy 21 or partial trisomy 21. Most (90%–95%) cases are caused by de novo chromosomal nondisjunction. About 2% to 6% of cases are caused by translocations of 2 chromosome 21s or a Robertsonian translocation of chromosome 21 fused to another acrocentric chromosome. Another 2% to 3% of cases are mosaic for trisomy 21. The prevalence of this disorder is 1/700 live births, but the risk of having a child with Down syndrome greatly increases with the age of the mother. The risk is 1/1000 at age 30 years and increases to 9/1000 at age 40 years.
Clinical features
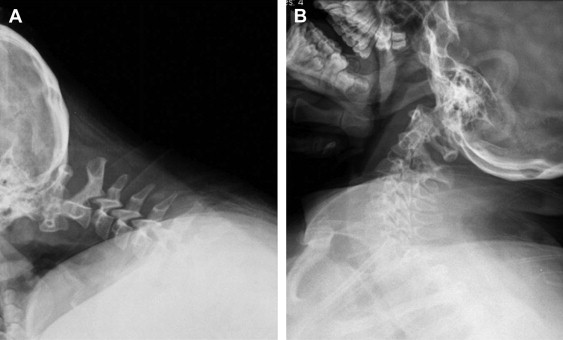
The main features of Down syndrome include cognitive impairment, hypotonia, and characteristic facial features. The IQ of individuals with trisomy 21 is highly variable, and most individuals fall between the moderate to severe range. IQ is not stable and decreases with age. Specific cognitive weaknesses have been identified in expressive language, syntactic/morphosyntactic processing, and verbal working memory. Craniofacial features include brachycephaly, midface hypoplasia, flat or depressed nasal bridge, micrognathia, and epicanthic folds ( Fig. 1 ). In addition, there are outer (dysmorphic outer ear and stenosis of the external ear canal), middle (malformation of the eustachian tube), and inner ear anomalies, which can result in hearing loss and cholesteatoma. Dental issues include variable tooth morphogenesis and eruption and a greater prevalence and severity of periodontal disease, but lower incidence of caries. Changes in the oral cavity include macroglossia and a protruding furrowed tongue as well as narrow palate, pharynx, and oropharynx. Many of these craniofacial issues can lead to sleep apnea, and because of a decrease of immune function in individuals with Down syndrome, these can also lead to chronic infections. Congenital heart defects are not present in all individuals but contribute greatly to mortality. These anomalies include atrioventricular canal defect, tetralogy of Fallot, and patent ductus arteriosus but particularly atrioventricular septal defects. There are many confounding issues with individuals with trisomy 21. There is a greater risk for leukemia, both acute lymphoblastic leukemia and acute myelogenous leukemia. Approximately 45% of individuals with Down syndrome age 45 years or older develop Alzheimer-related dementia. Individuals with trisomy 21 also have an increased risk of atlantoaxial instability ( Fig. 2 ). The phenotype can be variable in individuals with mosaic Down syndrome. The average life expectancy is 49 years in the white population, although there is racial disparity.

Differential diagnosis
Trisomy 18 is an aneuploidy that manifests in severe cognitive delay and heart problems but may also have problems in the digestive, reproductive, and urologic systems. The disorder is often fatal in infancy or early childhood. Males with more than 1 X chromosome also have cognitive delay, distinct facies, and skeletal problems. Individuals with isolated hypotonia have no other distinctive features and have a normal chromosomal complement. Zellweger syndrome, a disease of peroxisome, also presents with hypotonia, cardiac defects, flat occiput and face, epicanthal folds, and palmer crease, similar to Down syndrome. Differential diagnosis can be made because individuals also present with congenital cataracts, hepatomegaly, contractures, and increased levels of iron and long-chain fatty acids. They also have a normal chromosomal complement. Autism manifests in general development delay in early childhood. A diagnosis of Down syndrome can be made using karyotype analysis or array comparative genomic hybridization.
Treatment considerations for the oral and maxillofacial surgeon
Atlantoaxial instability affects between 10% and 30% of individuals with Down syndrome, only 1.5% of whom need surgical intervention. Os odontoideum has been specifically associated with cervical instability, with the need for surgical intervention. To prevent any additional problems, radiologic evaluation of the cervical spine should be performed before any procedures requiring anesthesia. The neck should be maintained in a neutral position to prevent any extreme flexion, extension, or rotation. Tracheal stenosis can be more common in children with Down syndrome, which can lead to complications in anesthesia during surgery, such as complicated intubation or greater airway narrowing after intubation or bronchoscopy. Comprehensive assessment, including cardiac assessment, should be performed before surgery. Residual cardiac defects such as conduction disturbances and atrial rhythm anomalies can persist throughout the life of the individual, even after successful cardiac repair. Complications such as recurrent infections and a higher incidence of pulmonary hypertension, which contribute to increased mortality and morbidity, can also arise.
Down syndrome
Genetics
Down syndrome is the most frequently observed chromosomal aneuploidy caused by trisomy 21 or partial trisomy 21. Most (90%–95%) cases are caused by de novo chromosomal nondisjunction. About 2% to 6% of cases are caused by translocations of 2 chromosome 21s or a Robertsonian translocation of chromosome 21 fused to another acrocentric chromosome. Another 2% to 3% of cases are mosaic for trisomy 21. The prevalence of this disorder is 1/700 live births, but the risk of having a child with Down syndrome greatly increases with the age of the mother. The risk is 1/1000 at age 30 years and increases to 9/1000 at age 40 years.
Clinical features
The main features of Down syndrome include cognitive impairment, hypotonia, and characteristic facial features. The IQ of individuals with trisomy 21 is highly variable, and most individuals fall between the moderate to severe range. IQ is not stable and decreases with age. Specific cognitive weaknesses have been identified in expressive language, syntactic/morphosyntactic processing, and verbal working memory. Craniofacial features include brachycephaly, midface hypoplasia, flat or depressed nasal bridge, micrognathia, and epicanthic folds ( Fig. 1 ). In addition, there are outer (dysmorphic outer ear and stenosis of the external ear canal), middle (malformation of the eustachian tube), and inner ear anomalies, which can result in hearing loss and cholesteatoma. Dental issues include variable tooth morphogenesis and eruption and a greater prevalence and severity of periodontal disease, but lower incidence of caries. Changes in the oral cavity include macroglossia and a protruding furrowed tongue as well as narrow palate, pharynx, and oropharynx. Many of these craniofacial issues can lead to sleep apnea, and because of a decrease of immune function in individuals with Down syndrome, these can also lead to chronic infections. Congenital heart defects are not present in all individuals but contribute greatly to mortality. These anomalies include atrioventricular canal defect, tetralogy of Fallot, and patent ductus arteriosus but particularly atrioventricular septal defects. There are many confounding issues with individuals with trisomy 21. There is a greater risk for leukemia, both acute lymphoblastic leukemia and acute myelogenous leukemia. Approximately 45% of individuals with Down syndrome age 45 years or older develop Alzheimer-related dementia. Individuals with trisomy 21 also have an increased risk of atlantoaxial instability ( Fig. 2 ). The phenotype can be variable in individuals with mosaic Down syndrome. The average life expectancy is 49 years in the white population, although there is racial disparity.
Differential diagnosis
Trisomy 18 is an aneuploidy that manifests in severe cognitive delay and heart problems but may also have problems in the digestive, reproductive, and urologic systems. The disorder is often fatal in infancy or early childhood. Males with more than 1 X chromosome also have cognitive delay, distinct facies, and skeletal problems. Individuals with isolated hypotonia have no other distinctive features and have a normal chromosomal complement. Zellweger syndrome, a disease of peroxisome, also presents with hypotonia, cardiac defects, flat occiput and face, epicanthal folds, and palmer crease, similar to Down syndrome. Differential diagnosis can be made because individuals also present with congenital cataracts, hepatomegaly, contractures, and increased levels of iron and long-chain fatty acids. They also have a normal chromosomal complement. Autism manifests in general development delay in early childhood. A diagnosis of Down syndrome can be made using karyotype analysis or array comparative genomic hybridization.
Treatment considerations for the oral and maxillofacial surgeon
Atlantoaxial instability affects between 10% and 30% of individuals with Down syndrome, only 1.5% of whom need surgical intervention. Os odontoideum has been specifically associated with cervical instability, with the need for surgical intervention. To prevent any additional problems, radiologic evaluation of the cervical spine should be performed before any procedures requiring anesthesia. The neck should be maintained in a neutral position to prevent any extreme flexion, extension, or rotation. Tracheal stenosis can be more common in children with Down syndrome, which can lead to complications in anesthesia during surgery, such as complicated intubation or greater airway narrowing after intubation or bronchoscopy. Comprehensive assessment, including cardiac assessment, should be performed before surgery. Residual cardiac defects such as conduction disturbances and atrial rhythm anomalies can persist throughout the life of the individual, even after successful cardiac repair. Complications such as recurrent infections and a higher incidence of pulmonary hypertension, which contribute to increased mortality and morbidity, can also arise.
Klinefelter syndrome
Genetics
Klinefelter syndrome is the most common sex chromosome aneuploidy in males and is caused by having 1 extra X chromosome (47,XXY) (89.9%). Additional X chromosomes can also be present (48,XXXY [1.1%]; 49,XXXXY [1.8%]), and mosaicism can also exist (46,XY/47,XXY [6.6%]; 47,XXY/48,XXXY [0.2%]). The prevalence was 1 in 660 men in a Danish population. The risk increases with maternal age. The disorder is sporadic and usually caused by meiotic or mitotic nondisjunction in germ cells or in the fetus, respectively.
Clinical features
The 2 main features found in individuals with Klinefelter syndrome are hypergonadotropic hypogonadism with adults presenting with a high ratio of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) levels when compared with their testosterone levels and small testicular volume. Tall stature was believed to be a hallmark of the disorder, and growth in childhood and adolescence is accelerated, but mean adult height of affected men is 184.7 cm, which is not greatly different from the mean adult height of unaffected men (182.6 cm) in Denmark. Cryptorchidism (14%), gynecomastia (44%), and behavioral and learning problems (36%) are also observed, but not in all individuals. Verbal processing seems to be specifically affected. Other variable features include eunuchoid body habitus, long arms and legs, sparse body hair, and mandibular prognathism ( Fig. 3 ). This variable phenotype is seen in Fig. 4 , which shows an atypical phenotypic presentation. Individuals with Klinefelter syndrome are also at increased risk for metabolic syndrome, osteopenia/osteoporosis, breast cancer, autoimmune disorders, and mortality. Individuals with more X chromosomes seem to have a more severe phenotype, including additional congenital malformations and greater cognitive involvement.


