Introduction
The purpose of this study was to evaluate the change in natural head position (NHP) after orthognathic surgery in skeletal Class III patients.
Methods
We used pretreatment (T1) and posttreatment (T2) cephalometric radiographs and T1 and T2 lateral facial photographs of 20 skeletal Class III patients (mean age, 21.6 years), with 20 skeletal Class I patients (mean age, 22.2 years) as the controls. The Class III patients had undergone mandibular setback surgery, and the patients in the control group had received conventional orthodontic treatment. All lateral facial photographs were recorded in NHP. The true vertical line (TVL) was transferred from the photograph to the cephalometric radiograph, and then the angle between the TVL and the Frankfort horizontal plane (TVL/FH) was measured. A t test and a paired t test were used to verify the differences between the 2 groups, and between the T1 and T2 measurements in each group.
Results
The mean TVL/FH at T1 was significantly greater in the Class III group than in the Class I group; this indicated that the Class III group showed head flexion. However, the mean TVL/FH of the Class III group decreased by −3.1° at T2; this indicated head extension, and it did not significantly differ from that of the Class I group. Nineteen of the 20 Class I patients showed minimal or no change in their TVL/FH (−1.5° to 1.5°) at T2. On the other hand, 6 of the 20 Class III patients showed more than a 4.5° decrease in their TVL/FH at T2.
Conclusions
Most of the Class I patients showed minimal or no change in their NHP at T2, but some Class III patients had changes in their NHP that tended toward head extension after mandibular setback surgery. Thus, soft tissue analysis using the TVL in NHP may not be reliable for some skeletal Class III patients who undergo mandibular setback surgery.
Highlights
- •
We evaluated natural head position (NHP) in Class III patients after orthognathic surgery.
- •
Mean angle between the true vertical line and Frankfort horizontal plane in the Class III group decreased by −3.1° after surgery.
- •
Class I patients showed little or no change in NHP after orthodontic treatment.
- •
NHP changed in some Class III patients after mandibular setback surgery.
- •
They had more head extension after surgery.
Since the introduction of cephalometric radiography, orthodontists have used cephalometric analysis to plan orthodontic treatment and to evaluate the treatment results. Intracranial structures have been considered stable reference landmarks. Consequently, the sella-nasion plane (SN plane) and the Frankfort horizontal plane (FH plane) have been most commonly used as horizontal reference planes. However, some authors have reported individual variations of intracranial landmarks.
Natural head position (NHP) is a standardized and reproducible position of the head in an upright posture when the visual axis is horizontal. Many reports have confirmed the reproducibility of the NHP. Cooke reported in a 5-year longitudinal study on the reproducibility of the NHP method errors of 1.9° after 1 to 2 hours, 2.3° after 3 to 6 months, and 3.0° after 5 years. Peng and Cooke also reported that NHP has been shown to be remarkably reproducible (to 2.2°) even after 15 years.
In 1981, Spradley et al suggested that the subnasale true vertical line (TVL) may provide a useful tool for research on the soft tissue changes associated with both orthodontic and orthognathic surgical treatments. Viazis and Lundström and Lundström reported a cephalometric analysis using the true horizontal line based on NHP. Arnett and Bergman presented an organized and comprehensive approach to facial analysis using the NHP for orthodontic and surgical treatments. In 1999, Arnett et al presented a new soft tissue cephalometric analysis tool using the subnasale TVL for diagnosis and treatment planning for orthognathic surgery. Sugawara and Kawamura also used a TVL 5 mm ahead of the subnasale for soft tissue analysis for planning the surgical treatment objective.
However, Vig et al suggested that orthognathic surgery most likely shifts the center of mass of the head, thereby affecting head position. Arnett and McLaughlin recommended adjusting the head position during NHP registration because patients with Class II and Class III facial types tend to compensate for their head position. However, evidence of this is lacking, and there is no information on how much adjustment is needed.
There have been a few studies on the changes in NHP after orthognathic surgery. In the studies of Wenzel et al and Achilleos et al, the surgical setback of the mandible was shown to have decreased the nasopharyngeal airway space and increased the craniocervical angulation. However, there was no information on the TVL change. In 1991, Phillips et al reported no significant change in NHP a year after 1-jaw surgery (mandibular setback) or 2-jaw surgery (maxillary intrusion and mandibular setback). However, their study had no control group, and the ear rods and the forehead positioner in the cephalostat might have affected the real NHP of the patients. In 2005, Savjani et al found no significant change in NHP after orthognathic surgery. However, their study focused only on the vertical changes in the face after orthognathic surgery. Kim reported no change in NHP immediately after orthognathic surgery, but there was no information on the classifications of the malocclusions, types of surgery, or a control group.
The literature review did not clarify whether there had been any changes in NHP after orthognathic surgery in Class III patients. If NHP changes after mandibular setback surgery, soft tissue analysis using TVL for the surgical treatment objective may yield an unsatisfactory facial profile. The purpose of this study was to evaluate the change in NHP after orthognathic surgery in skeletal Class III patients.
Material and methods
In this retrospective study, we used pretreatment (T1) and posttreatment (T2) lateral cephalometric radiographs and T1 and T2 lateral facial photographs. The T1 lateral cephalometric radiographs and facial photographs were taken at the beginning of the treatment, and the T2 data were recorded immediately after the removal of the orthodontic appliances. Twenty subjects in the Class III group (11 male, 9 female; age range, 15.8-41.5 years; mean age, 21.6 ± 5.7 years) were consecutively selected from the skeletal Class III patients who had undergone mandibular setback surgery from 2005 to 2012 at Gangneung-Wonju National University Dental Hospital in Korea, and had their T1 and T2 lateral facial photographs taken in NHP. Twenty subjects for the control group were selected from skeletal Class I patients (9 male, 11 females; age range, 16.7-37.3 years; mean age, 22.2 ± 4.5 years; ANB angle range, 0.4°-4.0°) who had received conventional orthodontic treatment, and had their T1 and T2 lateral facial photographs taken in NHP. The exclusion criteria for the control group were (1) temporomandibular disorder, (2) tonsillar hypertrophy, (3) mouth breathing, and (4) anterior open bite or crossbite. The sample is described in Table I . Eight patients in the control group were treated without extractions, and 12 were treated with 4 premolar extractions. Seven patients in the Class III group were treated without extractions; 8 were treated with 2 maxillary premolar extractions; 2 were treated with 1 unilateral maxillary premolar extraction; 2 were treated with 4 premolar extractions; and 1 patient was congenitally missing 2 maxillary lateral incisors. The mean duration of their postsurgical orthodontic treatment after their mandibular setback surgery was 10.4 months in the Class III group. The protocols of this study were approved by the ethics committee (number 2010-1-3) of Gangneung-Wonju National University Dental Hospital.
| Skeletal Class III (n = 20) | Control (n = 20) | |||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Age (y) | 21.6 | 5.7 | 22.3 | 4.6 |
| Treatment duration (y) | 2.6 | 1.1 | 2.2 | 0.5 |
| ANB (°) | −2.2 | 3.1 | 2.3 | 0.9 |
| Frankfort-mandibular plane angle (°) | 29.8 | 5.9 | 28.3 | 4.8 |
The patients were instructed to stand in their natural position and to stare at their own eyes reflected in a 60 × 90 cm mirror at a distance of 1 m so that their lateral facial photographs in NHP could be taken. They were instructed to maintain their habitual occlusion with maximum intercuspation and to relax their lips while their lateral facial photographs were taken. A metal chain with a pendulum was attached to the background to show the true vertical plane in the facial photograph. The angle formed by the metal chain and the E-line (a line through the nasal tip and soft tissue pogonion) was measured in the facial photograph ( Fig 1 ). This angle was transferred to the cephalometric tracing to draw the TVL.

Lateral cephalometric radiographs (CX-90SP; Asahi Roentgen Ind, Kyoto, Japan) of all the patients were taken in the patients’ habitual occlusion and with relaxed lips, with the same instructions as those when their lateral facial photographs were shot. Nineteen landmarks and 6 reference planes were traced on the cephalometric radiographs using acetate paper and 0.5-mm pencils. The SN and FH planes of the T1 cephalograms were transferred to the T2 cephalograms with cranial-base superimpositions. Then in each T1 and T2 tracing, 7 linear and 4 angular measurements were made using Quick Ceph Studio software (Quick Ceph Systems, San Diego, Calif), and 1 linear measurement and 3 angular measurements were manually made with a protractor and a digital caliper. The linear measurements were calibrated by considering the magnification ratio of the radiographs (110%). All measurements and analyses were performed by 1 examiner (D.C.).
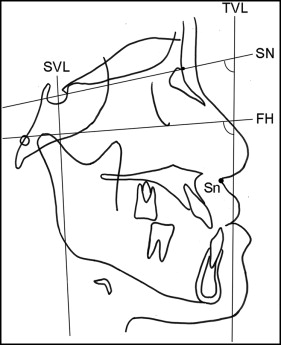
The measurement points and reference planes used in this study are shown in Figure 2 . The TVL was drawn to pass 5 mm ahead of subnasale. The angles between the TVL and SN plane (TVL/SN) and between the TVL and FH plane (TVL/FH) were evaluated to investigate the changes in NHP. In this study, the flexion and extension of the head in NHP were defined as an increase and a decrease in the TVL/SN and the TVL/FH, respectively. The distance from pogonion to a line perpendicular to the FH plane through sella (SVL) was measured to evaluate the amount of setback in the surgery group.
One examiner (D.C.) measured 10 randomly selected cephalometric radiographs and facial photographs, and repeated the TVL transfer and the cephalometric measurements 2 weeks later to determine the method errors of the cephalometric measurements. The method errors were calculated using Dahlberg’s formula (method error = √∑d2/2n
∑ d 2 / 2 n
, where d is the difference between the 2 measurements of a pair, and n is the number of samples). The maximum method errors of the measurements were 0.4 mm in mandibular length and 0.4° in TVL/FH. The intraexaminer correlation coefficients of the repeated measurements were greater than 0.963 (TVL-A′).
Statistical analysis
The normal distribution of the measurements was confirmed with the Shapiro-Wilk test ( P >0.05). The equality of the variances was checked using the Levene test. An independent t test was used to verify the difference between the mean values of the 2 groups. A paired t test was used to determine the differences between the T1 and T2 measurements in each group. Statistical significance was determined at the 5% level of confidence. All statistical analyses were performed with software (version 18.0; SPSS, Chicago, Ill).
Results
The T1 measurements between the groups are compared in Table II . The skeletal Class III group showed mandibular prognathism, concave profiles, and reverse overjets, unlike the control group. The mean TVL/SN and TVL/FH measurements were 83.1° and 91.8°, respectively, in the skeletal Class III group, and both were significantly greater than those in the control group (TVL/SN, 79.5°; TVL/FH, 88.3°).
| Variable | Skeletal Class III | Control | Class III vs Control | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | P value | Significance | |
| TVL/SN (°) | 83.1 | 3.6 | 79.5 | 3.5 | 0.002 | † |
| TVL/FH (°) | 91.8 | 3.6 | 88.3 | 3.8 | 0.005 | † |
| SNA (°) | 80.1 | 2.2 | 80.5 | 3.2 | 0.646 | NS |
| SNB (°) | 82.4 | 4.2 | 78.2 | 3.2 | 0.001 | † |
| ANB (°) | −2.2 | 3.1 | 2.3 | 0.9 | 0.000 | ‡ |
| Maxillary length (mm) | 82.4 | 4.6 | 83.9 | 4.2 | 0.296 | NS |
| Mandibular length (mm) | 120.9 | 7.8 | 113.4 | 6.2 | 0.002 | † |
| Pogonion to SVL (mm) | 66.0 | 9.2 | 57.2 | 6.0 | 0.001 | ‡ |
| Frankfort-mandibular plane angle (°) | 29.8 | 5.9 | 28.3 | 4.8 | 0.373 | NS |
| Lower anterior face height (mm) | 72.1 | 5.1 | 70.7 | 5.3 | 0.419 | NS |
| Overjet (mm) | −1.3 | 3.0 | 3.4 | 1.7 | 0.000 | ‡ |
| Overbite (mm) | 0.2 | 2.7 | 1.0 | 1.5 | 0.261 | NS |
| Upper lip to E-line (mm) | −3.3 | 2.8 | 0.9 | 1.9 | 0.000 | ‡ |
| Lower lip to E-line (mm) | 0.9 | 2.3 | 3.0 | 2.8 | 0.014 | ∗ |
| Facial contour angle (G′-Sn-Pog′) (°) | −1.1 | 6.8 | −9.9 | 3.6 | 0.000 | ‡ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


