
Management of ectodermal dysplasia I I—implant-retained removable prostheses
The use of dental implants in a growing child is not a routinely prescribed treatment approach. There is a paucity of data and studies on the growth pattern of the maxilla and mandible as it relates to the implant prosthesis in children. Since a child is still growing, placement of implants may interfere with or be affected by the continued growth of the maxilla and mandible. Therefore, implant therapy is currently a controversial form of prosthodontic care in a growing patient.Comprehensive treatment of pediatric patients with ectodermal dysplasia is somewhat controversial because their compromised dental state can be treated with conventional prostheses.
CASE STORY
A 6-year-old male patient with Rapp-Hodgkins anhidrotic ectodermal dysplasia presents for prosthodontic management of cleft palate and complete edentualism.
Figure 1: Frontal view.

Figure 2: Lateral view.

Figure 3: Maxillary occlusal view.

Figure 4: Mandibular occlusal view.

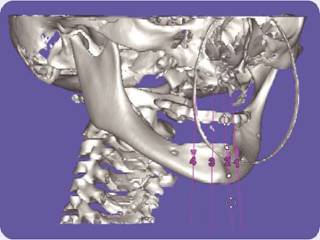
Figure 5: Computerized tomography.
LEARNING GOALS AND OBJECTIVES
- Understand the growth pattern of the maxilla and mandible in the growing patient.
- Understand the effects of anodontia and hypodontia.
- Understand the implication of implant prostheses in a growing child.
- Describe the importance of a maintenance program for young patients with ectodermal dysplasia with implant prostheses.
Medical History
- Rapp-Hodgkins anhidrotic ectodermal dysplasia
Dental History
- No previous dental treatment
Clinical Findings/Problem List
- Anodontia
- Cleft palate with oroantral fistula
- Edentulism
- Presence of mandibular tooth bud
Radiographic Findings
Figure 6: Panoramic radiograph.

Diagnosis
- Rapp-Hodgkins anhidrotic ectodermal dysplasia
- Anodontia
- Cleft palate
Clinical Decision-Making Determining Factors
- Anodontia refers to congenital absence of all teeth.
- Hypodontia is defined as partial congenital absence of teeth.
- Oral traits of ED may be expressed as anodontia or hypodontia with or without cleft lip and palate. Anodontia also manifests itself by lack of alveolar ridge development.
- Implant-supported prostheses or fixed partial dentures are avoided in young and actively growing patients because rigid fixed partial dentures could interfere with jaw growth, especially if the design crosses the midline (Pigno, Blackman et al.1996). The use of implants placed after age 15 years for girls and 18 years for boys were shown to have the most predictable prognosis. Because of the variation in growth among individuals, a prosthesis that provides retrievability is recommended for children. This facilitates and allows for adjustments related to growth and development (Cronin, Oesterle et al. 1994, 1998). Mandibular growth:
- The transverse growth of the mandible in the anterior region is finished before 1 year of age (Bjork 1964; Becktor, Becktor et al. 2001; Sharma and Vargervik 2006).
- The influence of edentulism on the growth of the mandible is not well understood. However, the insufficient vertical growth of the lower face and a reduced mandibular plane />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


