Case• 65. Failed endodontic treatment
SUMMARY
A 40-year-old lady presents to you with apical infection on a root-treated and crowned upper incisor. What are the treatment options and their likely chances of success?
History
Complaint
The patient, pointing to her upper right lateral incisor, complains that one of her crowns has fallen out. She is in no pain.
History of complaint
The crown fell out a few days ago. It has not fallen out before, though the adjacent crown on the upper right central incisor requires regular recementing.
Dental history
The patient has always attended regularly for dental treatment, but with a series of different practitioners. Some of the upper incisors were root treated about 10 years ago and all are crowned. Treatment was successful initially but she has suffered several episodes of pain over the last 5 years, for which she has been prescribed a number of courses of antibiotics. Periradicular surgery (apicectomy with root end filling) has been carried out on four occasions and she has suffered intermittent bouts of tenderness from most of the upper incisors since the last surgical procedure.
Medical history
The patient is otherwise fit and well.
Examination
Extraoral examination
The temporomandibular joints appear normal and no submental, submandibular or cervical lymph nodes are palpable.
Intraoral examination
The patient hands you a porcelain crown from the upper right lateral incisor with a cast gold post still cemented into it.
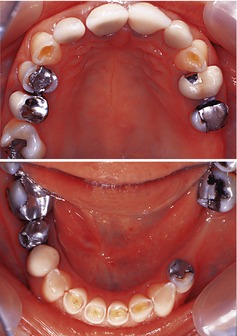
The appearances of the dentition with the crown temporarily reseated in the lateral incisor are shown in Figure 65.1 and in two occlusal views in Figure 65.2. There is tenderness over the apices of the central incisors, but not the right lateral incisor.
A sinus is present just above the mucogingival junction of the upper right central incisor. The likely causes would be a periapical abscess or chronic suppurative periradicular periodontitis, resulting from bacterial infection of a necrotic pulp or a failed endodontic treatment. Alternative causes include a periodontal abscess, perio-endo lesion or an infection associated with a root fracture.
There is slight erythema of the entire attached gingiva overlying the upper right central incisor root. This could be caused by a deep periodontal pocket, a perio-endo lesion or a fractured root.
All four upper incisor teeth are crowned and the crowns appear rather bulbous with poor marginal adaptation and contour.
The upper incisor crowns are spaced and irregular – note the upper left central incisor crown is wider than the right. It is possible that the natural dentition was spaced. Alternatively either periodontitis or bone loss from repeated surgery may have allowed some labial drift, though this seems unlikely because the teeth are not labially inclined. The spacing might also be the result of poor quality laboratory work.
There is marginal gingival inflammation around the upper incisors with a broad rounded gingival margin and little stippling. This is most probably caused by a combination of poor oral hygiene and plaque accumulation at the, possibly defective, margins of the crowns.
There is recession and loss of interdental papillae. This is probably also a result of plaque-induced inflammation. However, the gingival flap incision, which was necessary for periradicular surgery, might also have contributed and the tapering roots and wide interdental spaces of the upper incisors are prone to loss of interdental papillae when there is recession.
There is a faint scar line above the mucogingival junction of the upper incisors consistent with a healed submarginal semilunar flap, presumably made for periradicular surgery.
There is toothwear of the tips of the upper canines, lower incisors and canines and around the amalgam restorations in the lower arch. The lower incisors are worn to expose the reactionary dentine at the original site of the pulp. The toothwear is consistent with erosion (cupping out of the upper canines) and attrition (wear facets on lower incisors) due to the abrasive nature of the opposing porcelain crowns. For further discussion of toothwear see Case 60 and Case 61. It is possible that the upper incisors were crowned to overcome the cosmetic effect of toothwear – short crowns and sharp and flaking enamel at the incisal edges.
The gingival margin of the lower incisors is higher than that of the lower canines and premolars indicating that the lower incisors have overerupted, presumably as a result of the toothwear on upper and lower incisors.
Many of the posterior amalgam restorations have little contour and are ditched. However, this is no indication of clinical failure and they should not be replaced for this reason alone.

Investigations
▪ What investigations would you carry out and why?
Periodontal examination including recording of probing depths and gingival bleeding. It is necessary to identify whether there is pocket formation or only marginal inflammation. However, it will be difficult to assess the true attachment loss becaus/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


