Case• 30. Whose fault this time?
SUMMARY
You seem to be having trouble communicating with the dental laboratory. How will you tackle the problems that have arisen?
First patient
Complaint
Your nurse takes the special trays out of the laboratory package to record secondary impressions for an edentulous patient. They are not as special as you had intended.
History of complaint
You are constructing new complete dentures for a patient who has been a poor complete denture wearer. She has lost her lower denture and does not like the upper, so you have decided to make a new set from first principles rather than use a copy denture technique.
Primary impressions were recorded in stock trays adapted with silicone putty and covered with an alginate wash to record detail. You were going to take both upper and lower secondary impressions in close-fitting trays using zinc oxide and eugenol paste.
Diagnosis
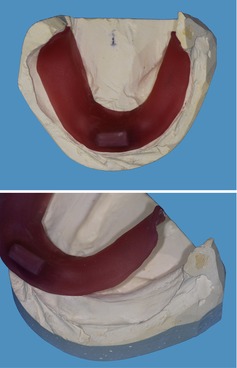
▪ The lower special trays are shown inFigures 30.1and30.2. What is wrong?
 |
| Fig. 30.1 |
 |
| Fig. 30.2 |
The tray is asymmetric: the extension on the patient’s left is considerably shorter than that on the right. However, when you look at the cast you see that your impression was short in that area and the laboratory has extended the tray as much as possible. They are correct not to have extended it over the land area in this region. The result is that it is underextended on the left buccal shelf. This is important because the lower denture will need to be extended here to gain good support.
Conversely, the tray has been overextended onto the land area in the floor of mouth and this will need to be altered prior to recording a secondary impression.
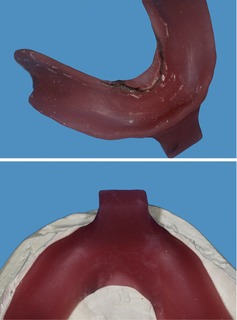
▪ The upper special tray is shown inFigure 30.3. What is wrong?
 |
| Fig. 30.3 |
This shows a well-constructed special tray, but it has been perforated and spaced for an alginate secondary impression. The tray is properly extended but spaced trays always look slightly overextended on a primary model because it sits lower after the spacer has been removed. Your heart sinks.
You look at the laboratory request sheet to see what you prescribed and read:
‘Please cast upper and lower primary impressions. Construct upper and lower special trays. N.B. lower close fitting for ZoE [zinc oxide and eugenol].’
Your diagnosis is poor communication. Many dentists and clinical dental technicians (CDTs) use alginate in a spaced tray for upper impressions. You had expected that the lab would assume that if one tray was close-fitting, then the other one would be too. You make a note to be more careful in future.
Solutions
▪ What can you do to save the patient a further appointment and yourself the additional cost of extra trays?
▪ What you can do about the upper tray?
There are a number of options but all have problems (Table 30.1). The only alternative would be to request a new tray.
| Possible solution | Disadvantages |
|---|---|
| Record the impression as planned with either zinc oxide and eugenol paste or an elastomeric material such as a medium-bodied addition-cured silicone | Will be impossible or certainly very messy to try |
| Record the impression with alginate | It is difficult to control the thickness of the rolled border with alginate. Unless you are using a modern 5-day-stable alginate, impressions need to be cast as soon as possible. Provided you use this material, this would be the best solution |
| Block perforations with composition or cold curing acrylic | Time-consuming but the tray would still have the wrong spacing for zinc oxide |
| Have a new tray made | Technically the best solution, but there are time and cost implications for the patient and you |
▪ What you can do about the lower tray?
This has one laboratory fault (overextension) and one fault resulting from your original impression (underextension). Again, you could take a new primary impression and request new special trays, but the lower tray is more easily dealt with. The best solution is to extend your tray in the buccal shelf using a material such as green or pink stick composition (pink is much easier to use as it flows at mouth temperature). The lingual overextension can be trimmed back with a bur to the correct extension, which is marked as a black line on the undersurface in the upper panel of Figure 30.2.
▪ What else should you check before trying to adapt the trays?
The extension should be checked in the patient’s mouth to ensure other areas are correct. Other common errors in tray construction relate to handle design. You need to check the handles to ensure they are properly constructed. Prosthodontists can become excited about tray handles but there are no absolute rules on what can and cannot be used. However, some tray handle designs could cause you and your patient problems.
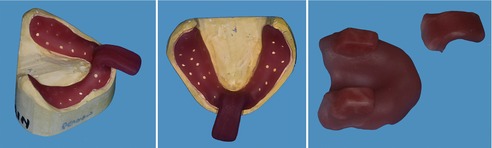
▪ Are these handles suitable?
From the appearances in Fig. 30.1, Fig. 30.2 and Fig. 30.3 the laboratory has provided well-made and designed handles. Faults to look for are shown in Figure 30.4. Can you identify them and the reasons why they are deficient?
 |
| Fig. 30.4 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


