Case• 15. Pain after extraction
SUMMARY
A 36-year-old lady presents with severe pain a few days after tooth extraction. What is the cause and what can be done?
History
Complaint
She complains of a distressingly severe pain from an extraction socket in the left side of her mandible. The pain is localized to the extraction socket and is not sensitive to hot or cold. It is a constant, dull, boring pain unrelieved by aspirin or paracetamol preparations. It prevents the patient performing any normal activity and kept her awake last night.
History of complaint
The patient underwent surgical removal of the lower left third molar tooth at her dentist 4 days ago. The extraction had proved more difficult than expected and involved repeated attempted elevation and a small amount of bone removal using a bur. Following the extraction, bleeding stopped normally. The extraction site had been tender but apparently was healing slowly until the pain started yesterday. Since then she has also noticed halitosis and a bad taste.
Medical history
The patient is otherwise fit and well. She is taking an oral contraceptive and no other positive findings were revealed by the medical history.
Examination
Extraoral examination
The patient has moderate extraoral swelling of the facial soft tissues overlying the extraction socket and some early discolouration of the skin by ecchymosis. There is trismus and she is able to open her mouth to only 22 mm interincisal clearance. There are no palpable lymph nodes in the deep cervical chain or submandibular triangle.
Intraoral examination
Halitosis is noticeable. The appearance of the socket is shown in Figure 15.1. The lower left third molar socket contains no tissue, only food debris. The surrounding soft tissues are slightly swollen but not significantly inflamed as judged by redness.
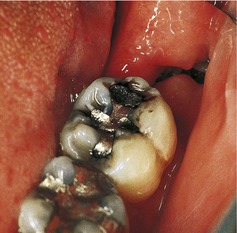 |
| Fig. 15.1 |
Diagnosis
▪ Based on what you know already, what is the most likely diagnosis?
The diagnosis is most likely to be a dry socket (alveolar osteitis). The history of severe and persistent pain localized to the tooth socket appearing 3–5 days after extraction, particularly a traumatic one, is characteristic. The lack of local inflammation or enlarged lymph nodes is compatible with this diagnosis and argues against post extraction infection either in the bone or soft tissue.
The diagnosis is confirmed by the examination which shows that the blood clot has been lost from the socket. In severe cases the bone of the socket may be exposed, and the bone of the distal lip of the socket can be seen in Figure 15.1.
Halitosis is the result of food debris in the socket being degraded by a partially anaerobic bacterial flora. The trismus is almost certainly related to the surgical trauma of extraction.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


