The development of an oral care path focuses on the identification of the early indicators of disease. Once the risks have been identified and diagnosed, the proper therapies can be selected and prescribed. The experienced practitioner must meld clinical experience and observation with evidence-based scientific dentistry and information on the treatment and prevention of continued disease for the prosthodontic patient after restorations have been completed. The incorporation of dental implants has not allowed for complications of caries and periodontal disease on teeth and implants. Osseoseparation is necessary for justification of continued maintenance.
Key points
- •
Current trends in dental disease management are centered on the identification or presence of disease and the mechanical elimination of the infected structures.
- •
The development of an oral care path redirects the focus on the identification of the early indicators of disease, before its existence. Once the risks have been identified and diagnosed, then the proper therapies can be selected and prescribed.
- •
The initial protocol of Featherstone’s research centered on the wide spectrum of caries, from white demineralized lesions to severe loss of tooth structure. He emphasized the effects of established preventive measures of xylitol, chlorhexidine, fluorides of increasing strengths, including varnish applications, and diet control.
- •
Some of the results are noncarious cervical lesions and some are caused by bacteria-induced inflammation, whereas others include bacteria-saturated harmful biofilm, which contributes to the effects on damaged tooth structure, lost supporting periodontium, multiple restorations, and missing teeth.
- •
The experienced practitioner must meld clinical experience and observation with rapidly evolving, evidence-based scientific dentistry and information on the treatment and prevention of continued disease for the prosthodontic patient after restorations have been completed.
- •
The incorporation of dental implants, once thought of as a 98% successful procedure, has not allowed for complications of caries and periodontal disease on teeth and implants. Thus, osseoseparation is necessary for justification of continued maintenance.
Introduction
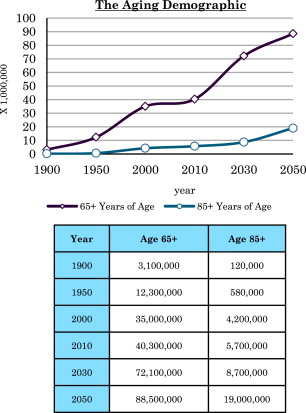
Current evidence-based dentistry studies on caries control in children (ref.) have changed the standard of care from the pediatric dental specialty to the medical model of infectious disease. Featherstone and colleagues have a renewed interest in caries management for all patients, beyond the boundaries of pediatric dentistry, from the young to the elderly. The Baby Boomer generation combines a population of health care–dependent and pharmacologically reliant aging individuals. In 2010, the population was estimated to have 40.3 million people 65 years of age and older, and was projected to reach 88.5 million individuals by 2050, a growth of nearly 20%. This paradigm shift has significant implications for the need and demand for general and oral health, and included in this demographic is the prosthodontic patient ( Fig. 1 ).
The management of oral and general health becomes more difficult as every decade progresses for these individuals. Hypertension, cholesterol, diabetes, depression, and decreased manual dexterity are among the more common medical conditions that afflict the aging. Caries continues to pose great challenges in prosthetic and restorative dentistry. Pjetursson and colleagues found that natural tooth abutment caries was the second most prevalent complication behind tooth devitalization. Goodacre and colleagues in an 8-year study found that there was a 27% incidence of failure with fixed partial dentures, of which 18% was caused by caries in the abutment teeth.
Most Common Fixed Partial Denture Complications
The largest obstacle for prosthodontics is not the fabrication of exceptional prosthetics but long-term supportive therapy to balance the risk factors for bacterial management ( Table 1 ).
| Cause of Failure | Number of Prostheses or Abutments Studied/Affected | Mean Incidence (%) |
|---|---|---|
| Caries | 3360/602 abutments | 18 |
| 1354/113 prostheses | 8 | |
| Need for endodontic treatment | 2514/276 abutments | 11 |
| 13576/88 prostheses | 7 | |
| Loss of retention | 1906/137 prostheses | 7 |
| Esthetics | 1024/58 prostheses | 6 |
| Periodontal disease | 1440/62 prostheses | 4 |
| Tooth fracture | 1602/44 prostheses | 3 |
| Prosthesis fracture | 1192/24 prostheses | 2 |
| Porcelain veneer fracture | 768/17 prostheses | 2 |
Prevention for the Prosthodontic Practice
For decades, as remains true, the 2 diseases that have accounted most for tooth loss are dental caries and periodontal disease. Evidence of tooth decay was recorded as far back as 5000 bc , when a tooth worm was described as the cause of the demineralization of dental enamel. The legend of the worm is also found in the writings of Homer, and as late as the 14th century ad , the surgeon Guy de Chauliac still promoted the belief that worms cause tooth decay. Current clinical studies have shown that caries is associated with increases in the proportions of acidogenic and aciduric (acid-tolerating) bacteria, especially streptococci (such as Streptococcus mutans and Streptococcus sobrinus ) and lactobacilli, which are capable of demineralizing enamel.
The role of caries management by risk assessment (CAMBRA) for the primary and secondary dentition identifies the causes of dental disease by assessing the degree of risk that an individual possesses and targeting the cause of caries, periodontal disease, recession, and xerostomia, for the prevention of tooth loss. Identification of these factors, which regulate the natural homeostasis present in plaque during health, but when disrupted drive the enrichment of oral pathogens, is crucial to the management of oral bacteria. Further manipulation of these ecologic influences could help maintain the beneficial microbial composition and normal metabolic activity of plaque biofilms and augment more conventional approaches to control caries ( Table 2 ).
| Common Risk Factors | |
|---|---|
|
|
|
|
A prosthodontic practice is not always exclusively comprehensive and restorative in nature, and often includes patients with removable and fixed appliances, special needs limitations, and developmental deficiencies. Prosthodontics has incorporated predictable dental implants into the established protocols of recent generations of restorative dentists, who previously had mainly concentrated on restoring and rerestoring damaged dentition. The application of ossseointegrated implants in restorative dentistry has contributed to the expanded role of prosthetic reconstruction. Long-term research for periodontal prosthetics, at the University of Pennsylvania, established the role of prosthodontics in the retention of the natural dentition with full and partial arch prosthetic restorations. The inclusion of combined interdisciplinary periodontal, endodontic, and prosthetic recall supportive therapy was essential to long-term supportive maintenance for success. Endodontic failure, prosthetic complication, and caries were implicated as major problems if periodontal therapy was successfully maintained.
The principles of informed consent remain a primary legal right for all patients to understand the risks and benefits of treatment options before allowing the removal of teeth that can be treated within their financial responsibilities. Informed patients can demand that every effort to retain as many of their natural teeth for as long as possible be considered an option. The specialty of prosthodontics is a cerebral specialty. As with all specialties, prosthodontics includes the knowledge of all available procedures within that specialty. It is just as important to know how and when to perform a procedure as well as when not to perform a procedure. It is essential to include the patient in a long-term program for supportive maintenance and control of the causes of the most common cause of prosthetic failure, caries.
Caries Initiation
Caries is a result of changes in the environment caused by acid production from the fermentation of dietary carbohydrates, which selects for acidogenic and acid-tolerating species such as mutans streptococci and lactobacilli.
In any ecosystem, homeostasis can break down on occasion because of a substantial change in a parameter that is critical to maintaining ecologic stability at a site.
The formation of the pellicle on the tooth surface is the first and most important step of the bacteria colonization process (Fig. 5.1). The pellicle acts as a protective layer to slow the diffusion of acid as well as being a reservoir for calcium and phosphate. It also acts as an attachment catalyst for early bacterial colonizers, Streptococcus sobrinus and Actinomyces viscosus .
The polysaccharide surface proteins produced by these bacteria enable cell to pellicle surface adhesion, which in turn attracts the attachment of S mutans , and the opportunistic colonization of lactobacilli. These bacteria can rapidly metabolize dietary sugars to acid, creating locally a low pH. These organisms multiply and metabolize optimally at low pH. Under such conditions, they become more competitive, whereas most species associated with enamel health are sensitive to acidic environmental conditions. Carious disease could be prevented not only by targeting the pathogens directly but also by interfering with the key environmental factors driving the deleterious ecologic shifts in the composition of the plaque biofilms.
Introduction
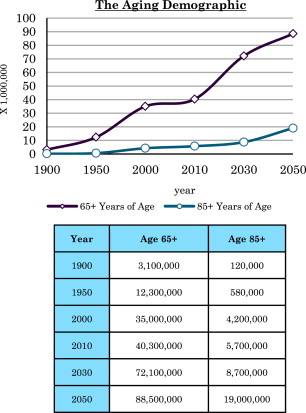
Current evidence-based dentistry studies on caries control in children (ref.) have changed the standard of care from the pediatric dental specialty to the medical model of infectious disease. Featherstone and colleagues have a renewed interest in caries management for all patients, beyond the boundaries of pediatric dentistry, from the young to the elderly. The Baby Boomer generation combines a population of health care–dependent and pharmacologically reliant aging individuals. In 2010, the population was estimated to have 40.3 million people 65 years of age and older, and was projected to reach 88.5 million individuals by 2050, a growth of nearly 20%. This paradigm shift has significant implications for the need and demand for general and oral health, and included in this demographic is the prosthodontic patient ( Fig. 1 ).
The management of oral and general health becomes more difficult as every decade progresses for these individuals. Hypertension, cholesterol, diabetes, depression, and decreased manual dexterity are among the more common medical conditions that afflict the aging. Caries continues to pose great challenges in prosthetic and restorative dentistry. Pjetursson and colleagues found that natural tooth abutment caries was the second most prevalent complication behind tooth devitalization. Goodacre and colleagues in an 8-year study found that there was a 27% incidence of failure with fixed partial dentures, of which 18% was caused by caries in the abutment teeth.
Most Common Fixed Partial Denture Complications
The largest obstacle for prosthodontics is not the fabrication of exceptional prosthetics but long-term supportive therapy to balance the risk factors for bacterial management ( Table 1 ).
| Cause of Failure | Number of Prostheses or Abutments Studied/Affected | Mean Incidence (%) |
|---|---|---|
| Caries | 3360/602 abutments | 18 |
| 1354/113 prostheses | 8 | |
| Need for endodontic treatment | 2514/276 abutments | 11 |
| 13576/88 prostheses | 7 | |
| Loss of retention | 1906/137 prostheses | 7 |
| Esthetics | 1024/58 prostheses | 6 |
| Periodontal disease | 1440/62 prostheses | 4 |
| Tooth fracture | 1602/44 prostheses | 3 |
| Prosthesis fracture | 1192/24 prostheses | 2 |
| Porcelain veneer fracture | 768/17 prostheses | 2 |
Prevention for the Prosthodontic Practice
For decades, as remains true, the 2 diseases that have accounted most for tooth loss are dental caries and periodontal disease. Evidence of tooth decay was recorded as far back as 5000 bc , when a tooth worm was described as the cause of the demineralization of dental enamel. The legend of the worm is also found in the writings of Homer, and as late as the 14th century ad , the surgeon Guy de Chauliac still promoted the belief that worms cause tooth decay. Current clinical studies have shown that caries is associated with increases in the proportions of acidogenic and aciduric (acid-tolerating) bacteria, especially streptococci (such as Streptococcus mutans and Streptococcus sobrinus ) and lactobacilli, which are capable of demineralizing enamel.
The role of caries management by risk assessment (CAMBRA) for the primary and secondary dentition identifies the causes of dental disease by assessing the degree of risk that an individual possesses and targeting the cause of caries, periodontal disease, recession, and xerostomia, for the prevention of tooth loss. Identification of these factors, which regulate the natural homeostasis present in plaque during health, but when disrupted drive the enrichment of oral pathogens, is crucial to the management of oral bacteria. Further manipulation of these ecologic influences could help maintain the beneficial microbial composition and normal metabolic activity of plaque biofilms and augment more conventional approaches to control caries ( Table 2 ).
| Common Risk Factors | |
|---|---|
|
|
|
|
A prosthodontic practice is not always exclusively comprehensive and restorative in nature, and often includes patients with removable and fixed appliances, special needs limitations, and developmental deficiencies. Prosthodontics has incorporated predictable dental implants into the established protocols of recent generations of restorative dentists, who previously had mainly concentrated on restoring and rerestoring damaged dentition. The application of ossseointegrated implants in restorative dentistry has contributed to the expanded role of prosthetic reconstruction. Long-term research for periodontal prosthetics, at the University of Pennsylvania, established the role of prosthodontics in the retention of the natural dentition with full and partial arch prosthetic restorations. The inclusion of combined interdisciplinary periodontal, endodontic, and prosthetic recall supportive therapy was essential to long-term supportive maintenance for success. Endodontic failure, prosthetic complication, and caries were implicated as major problems if periodontal therapy was successfully maintained.
The principles of informed consent remain a primary legal right for all patients to understand the risks and benefits of treatment options before allowing the removal of teeth that can be treated within their financial responsibilities. Informed patients can demand that every effort to retain as many of their natural teeth for as long as possible be considered an option. The specialty of prosthodontics is a cerebral specialty. As with all specialties, prosthodontics includes the knowledge of all available procedures within that specialty. It is just as important to know how and when to perform a procedure as well as when not to perform a procedure. It is essential to include the patient in a long-term program for supportive maintenance and control of the causes of the most common cause of prosthetic failure, caries.
Caries Initiation
Caries is a result of changes in the environment caused by acid production from the fermentation of dietary carbohydrates, which selects for acidogenic and acid-tolerating species such as mutans streptococci and lactobacilli.
In any ecosystem, homeostasis can break down on occasion because of a substantial change in a parameter that is critical to maintaining ecologic stability at a site.
The formation of the pellicle on the tooth surface is the first and most important step of the bacteria colonization process (Fig. 5.1). The pellicle acts as a protective layer to slow the diffusion of acid as well as being a reservoir for calcium and phosphate. It also acts as an attachment catalyst for early bacterial colonizers, Streptococcus sobrinus and Actinomyces viscosus .
The polysaccharide surface proteins produced by these bacteria enable cell to pellicle surface adhesion, which in turn attracts the attachment of S mutans , and the opportunistic colonization of lactobacilli. These bacteria can rapidly metabolize dietary sugars to acid, creating locally a low pH. These organisms multiply and metabolize optimally at low pH. Under such conditions, they become more competitive, whereas most species associated with enamel health are sensitive to acidic environmental conditions. Carious disease could be prevented not only by targeting the pathogens directly but also by interfering with the key environmental factors driving the deleterious ecologic shifts in the composition of the plaque biofilms.
Xerostomia
The production and presence of saliva are crucial in maintaining the health of the oral soft tissues and providing antimicrobial and pH buffering effects. A normal flow of 1.5 L per day contains calcium and phosphate, bicarbonate, immunoglobins, mucins, and proteins, all of which are essential in contributing to the remineralization of tooth enamel and the neutralization of acids in the oral cavity ( Table 3 ). Reduced salivary flow can be a result of damaged salivary glands but is commonly an associated side effect of various medical conditions; uncontrolled diabetes, chemotherapy, head and neck radiation, and autoimmune disorders.
| Commonly Prescribed Medications | |||
|---|---|---|---|
|
|
|
|
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


