This case report describes the successful treatment of an adult with a skeletal Class II Division 2 posttraumatic dentition with consequential restorations. The extracted maxillary premolar was autotransplanted to replace the hopeless mandibular first molar. The endodontically treated maxillary right canine was extracted instead of the premolar. A multidisciplinary approach including autotransplantation and orthodontic treatment provided a satisfactory outcome.
Trauma can result in fractures of the facial bones, alveolar bones, and the teeth, along with the loss of multiple teeth. During multidisciplinary reconstruction procedures, we sometimes confront unwanted iatrogenic complications, poor prognoses, or unsatisfying treatment outcomes.
Here, we report the orthodontic treatment of an adult patient with a Class II malocclusion and severe crowding. Because of trauma and previous reconstruction therapy, there were multiple dental implants, tooth fractures, and endodontically treated teeth. In addition, a molar was hopeless as a result of periodontal problems. An unusual extraction regimen was applied by extracting the endodontically treated maxillary canine instead of the dental implant, and the other extracted premolar was autotransplanted to replace the extracted mandibular molar.
Diagnosis and etiology
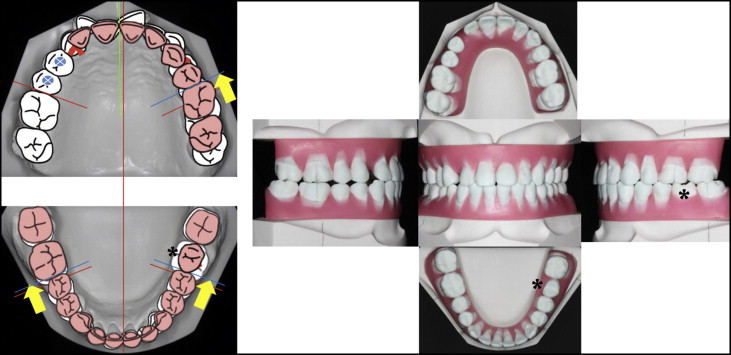
A 37-year-old woman was referred by her periodontist for evaluation and treatment of her malocclusion. After trauma 4 years previously, her maxillary right premolars were avulsed and replaced with dental implants. Her mandibular left first molar had a periodontal abscess, Class III furcation involvement, probing depths over 6 mm, a crack in the mesial root, and distal root caries with a periapical lesion. After diagnostic surgery, the first molar was diagnosed as hopeless by the periodontist. When the periodontist first met the patient, he was concerned that although implants and restorations were placed to restore the avulsed teeth, they were not functionally in contact with the mandibular dentition. Furthermore, the patient had an unesthetic smile caused by severe crowding, which was her chief complaint ( Figs 1 and 2 ).

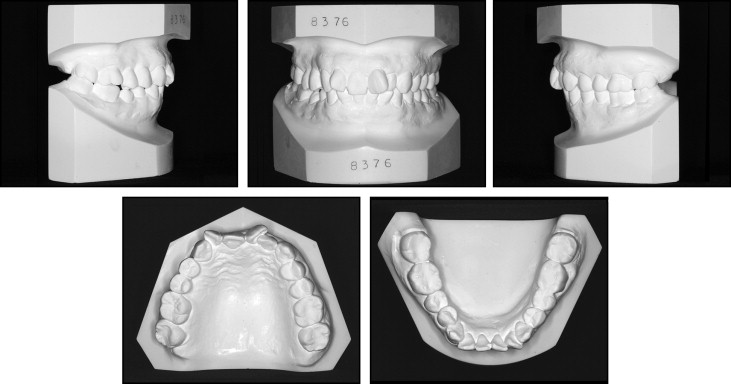
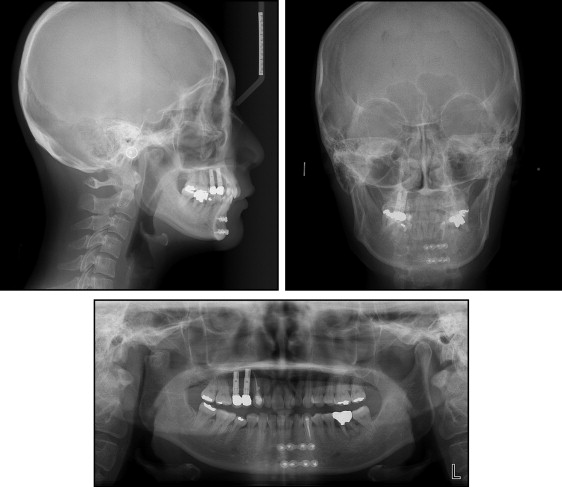
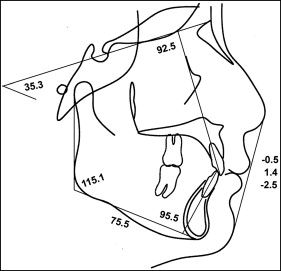
The patient had moderate to severe crowding. Both the skeletal and dental relationships were Class II, and the profile was straight ( Figs 1 and 2 ). According to the panoramic radiograph, the mandibular left first molar had furcation involvement with a periapical lesion, and the maxillary right premolars were restored with dental implants. Although a malunion of the right condyle was noted, there was no restriction in mandibular motion. The cephalometric radiographs showed a retrusive mandible (SNB angle, 70.8°) compared with a relatively well-positioned maxilla (SNA angle, 76.2°), indicating a skeletal Class II malocclusion (ANB angle, 5.4°). The maxillary incisors were retroclined (U1-SN, 92.5°). Vertically, the patient was normodivergent (SN-MP, 35.3°). The mandible was slightly deviated to the right side ( Figs 3 and 4 ; Table ).
| Variable | Norm | Pretreatment | Posttreatment |
|---|---|---|---|
| Skeletal | |||
| SNA (°) | 81.6 | 76.2 | 76.3 |
| SNB (°) | 79.1 | 70.8 | 70.9 |
| ANB (°) | 2.4 | 5.4 | 5.5 |
| FMA (°) | 24.0 | 21.7 | 22.0 |
| Gonial angle (°) | 118.6 | 115.1 | 115.3 |
| SN-MP (°) | 34.0 | 35.3 | 35.5 |
| Ramus height (mm) | 51.6 | 46.5 | 46.5 |
| Body length (mm) | 76.0 | 75.5 | 75.5 |
| Facial height ratio | 66.0 | 64.3 | 64.2 |
| Dental | |||
| U1-SN (°) | 106.0 | 92.5 | 94.5 |
| IMPA (°) | 94.0 | 95.5 | 98.5 |
| Interincisal angle (°) | 126.0 | 129.3 | 127.0 |
| Occlusal plane | 15.0 | 12.9 | 13.0 |
| Soft tissues | |||
| Upper lip to E-plane | −1.0 | −0.5 | −2.5 |
| Lower lip to E-plane | 1.0 | −2.5 | −3.0 |
From her medical records, we learned that as a result of trauma 4 years previously, her right condyle and mandibular body were fractured, the maxillary right premolars were avulsed, the mandibular right canine was fractured, and the mandibular left canine was nonvital. The maxillary right canine had most likely been punctured with bone screws during the intermaxillary fixation procedure. Afterward, the premolars were restored with dental implants, and the maxillary right and mandibular left canines were endodontically treated. The mandibular right canine was left untreated because its vitality and mobility were within normal limits, with no specific symptoms. Unrelated to the trauma, the endodontic treatment of the mandibular left first molar was incomplete with a periapical lesion and furcation involvement ( Fig 5 ).

According to our evaluation of the orthodontic records and her history, the patient was diagnosed with a skeletal Class II Division 2 malocclusion and severe crowding.
Treatment alternatives
Under normal circumstances, extraction of the 2 maxillary first premolars would have been considered to relieve the crowding. Afterward, the maxillary molars would be protracted, and the mandibular dentition would be distalized to finish with complete Class II molar and Class I canine relationships with no evident changes in the profile. However, because of the preexisting dental implants on the maxillary right side, premolar extraction and movement of the maxillary right molar segment was not an option. Therefore, we decided to extract the endodontically treated maxillary right canine instead of the maxillary right premolar in addition to the left first premolar. After relieving the crowding, the remaining space on the right side would be restored with prosthetics for esthetic reasons. Meanwhile, the mandibular right molar region could be uprighted and distalized to relieve the premolar crowding.
The prognosis for movement of the mandibular right canine was questionable because of a fracture line, even though the tooth showed no signs or symptoms, and mobility was within normal limits. Fortunately, according to the treatment plan, major tooth movement in the mesiodistal or vertical direction was not necessary for the mandibular right canine, so we decided to level the canine under close monitoring. After orthodontic treatment, the hopeless left molar could be replaced with a dental implant.
An alternative treatment option would be to replace the hopeless mandibular molar with an extracted maxillary first premolar via autotransplantation, and the maxillary arch would be treated in the same fashion as the first option. In this case, an additional dental implant would not be necessary to restore the mandibular molar. Since the recipient site had enough space, extraction and autotransplantation could be done on the same day, thereby reducing treatment time rather than finishing with a dental implant after orthodontic treatment. Using 3-dimensional imaging and a diagnostic setup, we planned to rotate the autotransplant 90° during transplantation to gain a mesiodistal dimension similar to the extracted first molar ( Fig 6 ).