Introduction
The aim of this study was to compare dental arch-width and perimeter changes in patients with borderline Class I occlusion, treated with extractions or without extractions with air-rotor stripping (ARS).
Methods
The study was conducted with 26 sets of pretreatment and posttreatment dental models of patients with borderline Class I occlusion. Thirteen patients (mean age, 18.1 ± 3.7 years) were treated with 4 premolar extractions, and 13 (mean age, 17.8 ± 2.4 years) were treated without extractions but with the ARS technique. Mean maxillary and mandibular crowding values were 5.7 ± 1.5 and 5.9 ± 1.4 mm in the extraction group, and 5.0 ± 1.3 and 5.9 ± 1.3 mm in the nonextraction group, respectively. A digital caliper was used to measure maxillary and mandibular intercanine and intermolar arch widths and arch perimeters. The Wilcoxon test was used to evaluate treatment changes in each group. The Mann-Whitney U test was used to compare the pretreatment and posttreatment values and the treatment changes between the 2 groups.
Results
At the start of treatment, the maxillary and mandibular intercanine and intermolar widths and the arch perimeters of both groups did not differ statistically. The maxillary intercanine widths were maintained in both groups. The maxillary and mandibular intermolar widths and arch perimeters decreased in the extraction group. In the nonextraction group, intermolar widths decreased, but arch perimeters did not change significantly. After treatment, the maxillary and mandibular intercanine widths were not different between the groups.
Conclusions
In Class I borderline patients with moderate crowding, extraction therapy with minimum anchorage did not result in narrower dental arches, and nonextraction treatment with ARS preserved the intercanine arch widths and arch perimeters.
The consequences of extraction and nonextraction therapies in various maloclusions have been widely investigated. In addition to hard- and soft-tissue changes after extraction and nonextraction, arch-width changes are also discussed by orthodontists. Dimensional changes of the dental arch gained attention because of their possible influences on smile esthetics and long-term stability.
Some authors claimed that extraction treatment resulted in constricted arch forms with narrower dental arch widths and reduced the fullness of the dentition during smiling, whereas others suggested that narrower dental arches and unesthetic smiles were unexpected.
In nonextraction treatment modalities, the resolution of crowding is usually achieved by distal movement of the posterior teeth, advancement of the anterior teeth, and transversal expansion. Tooth movement in 3 planes of space naturally leads to increased arch dimensions. In most studies conducted on patients with Class I malocclusions, it was shown that mandibular intercanine width increased after nonextraction treatment. On the other hand, significant expansion of the dental arches can adversely affect the stability of orthodontic treatment outcomes. The mandibular intercanine width has especially been considered immutable by some authors.
As an alternative to tooth extraction and various nonextraction treatment modalities in patients with moderate crowding, air-rotor stripping (ARS) was introduced by Sheridan. The space obtained by the removal of interproximal enamel is used to resolve the crowding without significant lateral expansion and incisor proclination. A recent prospective study evaluated the effects of extraction and nonextraction therapy with ARS on dentoskeletal structures and facial profiles in Class I borderline patients. However, no comparison of dental arch-width changes between the 2 treatment alternatives was reported in the literature.
The objective of this study was to assess arch-width and perimeter changes in Class I borderline patients treated with extraction or nonextraction with ARS.
Material and methods
The sample consisted of 26 borderline Angle Class I patients who could have been treated either with or without extraction because of their moderate dental arch crowding, balanced facial profiles, and dentoskeletal relationships. The selection criteria were (1) orthognathic facial profile, moderate maxillary and mandibular dental arch crowding, and Angle Class I molar relationship; (2) no skeletal discrepancy, constricted maxillary dental arch, posterior crossbite, or congenitally missing teeth; and (3) completed pubertal growth spurt.
The research was approved by the ethical committee of the Medical School of Hacettepe University, Ankara, Turkey.
Patients referred to the orthodontic clinic in a time period of 4 years were evaluated by experienced orthodontists according to their intraoral and extraoral photographs, and cephalometric and model analyses. Borderline patients meeting the selection criteria were informed about the 2 treatment alternatives: extraction and nonextraction with ARS. Informed consent was obtained from each patient before orthodontic treatment. Those who did not want to participate in this study were excluded. Patients who accepted treatment were randomly divided into 2 groups. In the order of referral to the orthodontic clinic, the first patient was assigned to the extraction group, and the next one to the nonextraction group. In the first group, 13 patients were treated with extraction of 4 premolars. Maxillary and mandibular first premolars were extracted in 10 patients, and maxillary and mandibular second premolars were extracted in 3 patients. In the second group, the crowding was resolved with the ARS technique. No expansion appliances were used in any group. The sex distribution, mean ages, treatment times, and dental crowding amounts of all subjects are shown in Table I .
| Group | Male (n) | Female (n) | Total (n) | Age (y) Mean ± SD | Treatment time (mo) Mean ± SD | Maxillary crowding (mm) Mean ± SD | Mandibular crowding (mm) Mean ± SD |
|---|---|---|---|---|---|---|---|
| Extraction | 2 | 11 | 13 | 18.1 ± 3.7 | 24.8 ± 6.9 | –5.7 ± 1.5 | –5.9 ± 1.4 |
| Nonextraction | 2 | 11 | 13 | 17.8 ± 2.4 | 17.0 ± 4.6 | –5.0 ± 1.3 | –5.9 ± 1.3 |
In the extraction group, after the premolar extractions, the treatment started with sectional canine distalization. No anchorage preparation was made during segmental canine distalization. After the elimination of crowding, the remaining extraction spaces were closed with increased labial crown torqued archwires. All anterior teeth were tied together to increase anterior anchorage and allow mesialization of the posterior teeth rather than retraction of the anterior teeth.
In the nonextraction group, before ARS, the enamel thickness of the teeth was evaluated on bite-wing radiographs. The ARS technique was applied to posterior and anterior teeth with a specially designed ARS bur kit (Raintree Essix, Metairie, La). A segmental approach was preferred to eliminate the excessive protrusion of the incisors. At the beginning of orthodontic treatment, the posterior teeth were leveled, and separators were placed between the first molars and second premolars. After separation, the enamel on the mesial side of the first molars and the distal side of the second premolars was reduced with 699 LC crosscut fissure tungsten carbide burs (Raintree Essix) and finished with finishing diamond burs and Extrathin medium and fine Sof-Lex polishing disks (3M Dental Products, St Paul, Minn). With the combination of anterior Essix plate to reinforce anterior anchorage, the second premolars were distalized by using open push coils into the space obtained by stripping. Then this procedure was continued from the posterior to the anterior teeth. When the canines were distalized, the incisors were bonded and stripped with fine diamond burs (55000, Raintree Essix). Topical fluoride gel was applied after stripping, and the subjects were advised to use fluoride mouth rinse during their orthodontic therapy.
At the end of extraction and nonextraction treatment, all patients were successfully treated (ie, they had good occlusion with Class I canine and molar relationships, and well-aligned and interdigitated arches with no crowding or remaining extraction spaces).
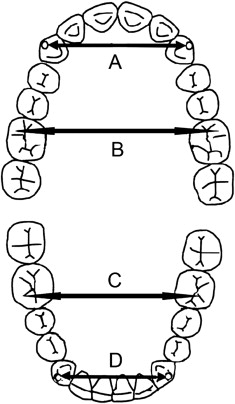
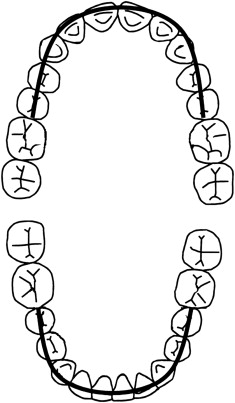
The intercanine and intermolar widths in the maxillary and mandibular arches were measured with a digital caliper (Opto-Rs 232 simplex/duplex, Sylvac/Fowler, Crissier, Switzerland) on study models. The cusp tips of the teeth were marked with a black 0.3-mm pencil. The distances between the mesiobuccal cusp tips of the molars (intermolar widths) and cusp tips of the canines (intercanine widths) were measured to determine the intermolar and intercanine widths on the pretreatment (T1) and posttreatment (T2) study models, as described by Kim and Gianelly ( Fig 1 ). Dental arch perimeters were measured between the mesial contact points of the first molars over the contact points of the posterior teeth and the incisal edges of the anterior teeth with a flexible ruler on the maxillary and mandibular dental casts ( Fig 2 ).
In both groups, arch widths and perimeters at T1 and T2 were recorded, and treatment changes were calculated as the differences between the T2 and the T1 measurements.
Statistical analysis
All statistical analyses were performed with the SPSS software package (SPSS for Windows 98, version 10.0, SPSS, Chicago, Ill). For each variable, the arithmetic mean and the standard deviation were calculated. The Wilcoxon test was used to evaluate treatment changes in each group. The Mann-Whitney U test was used to compare the T1 and T2 values and treatment changes between the groups. Statistical significance was established at P <0.05.
Two weeks after the first measurements, all variables were remeasured by the same examiner (S.A.). Random errors were calculated with Dahlberg’s formula. Method errors ranged from 0.15 to 0.62 mm.
Results
At T1, the maxillary and mandibular intercanine and intermolar widths and arch perimeters of the groups did not differ statistically ( Table II ).
| Measurement (mm) | Extraction (n = 13) Mean ± SD | Nonextraction (n = 13) Mean ± SD | P |
|---|---|---|---|
| Maxillary intercanine width | 35.01 ± 3.66 | 34.02 ± 2.98 | 0.442 |
| Maxillary intermolar width | 50.48 ± 2.49 | 50.49 ± 2.79 | 0.939 |
| Maxillary arch perimeter | 73.38 ± 2.69 | 75.46 ± 4.91 | 0.098 |
| Mandibular intercanine width | 25.16 ± 1.65 | 24.60 ± 2.25 | 0.555 |
| Mandibular intermolar width | 43.54 ± 1.98 | 43.07 ± 3.29 | 0.521 |
| Mandibular arch perimeter | 63.31 ± 2.81 | 63.46 ± 3.91 | 0.757 |
At T2, the mean maxillary intercanine widths were maintained in both groups ( Table III ). The mean maxillary intermolar widths were significantly decreased in both groups (extraction, –2.23 ± 1.27 mm, P <0.01; nonextraction, –1.07 ± 1.19 mm, P <0.05) ( Table III ). The maxillary arch perimeter was significantly decreased in the extraction group, with a mean value of 8.23 ± 2.01 mm ( P <0.01), and it was maintained in the nonextraction group ( Table III ).
| Measurement (mm) | Time | Extraction (n = 13) Mean ± SD | P | Nonextraction (n = 13) Mean ± SD | P |
|---|---|---|---|---|---|
| Maxillary intercanine width | T1 | 35.01 ± 3.66 | 0.65 | 34.02 ± 2.98 | 0.78 |
| T2 | 35.16 ± 2.10 | 33.78 ± 2.04 | |||
| T2-T1 | 0.15 ± 2.59 | –0.24 ± 1.92 | |||
| Maxillary intermolar width | T1 | 50.48 ± 2.49 | 0.002 † | 50.49 ± 2.79 | 0.011 ∗ |
| T2 | 48.25 ± 2.05 | 49.42 ± 2.13 | |||
| T2-T1 | –2.23 ± 1.27 | –1.07 ± 1.19 | |||
| Maxillary arch perimeter | T1 | 73.38 ± 2.69 | 0.001 † | 75.46 ± 4.91 | 0.469 |
| T2 | 65.15 ± 3.51 | 75.15 ± 3.36 | |||
| T2-T1 | –8.23 ± 2.01 | –0.31 ± 2.29 | |||
| Mandibular intercanine width | T1 | 25.16 ± 1.65 | 0.019 ∗ | 24.60 ± 2.25 | 0.173 |
| T2 | 26.17 ± 1.55 | 25.52 ± 1.45 | |||
| T2-T1 | 1.01 ± 1.59 | 0.92 ± 2.01 | |||
| Mandibular intermolar width | T1 | 43.54 ± 1.98 | 0.001 † | 43.07 ± 3.29 | 0.046 ∗ |
| T2 | 40.38 ± 1.61 | 41.81 ± 2.34 | |||
| T2-T1 | –3.16 ± 1.13 | –1.26 ± 1.90 | |||
| Mandibular arch perimeter | T1 | 63.31 ± 2.81 | 0.001 † | 63.46 ± 3.91 | 0.214 |
| T2 | 54.76 ± 4.27 | 64.15 ± 3.05 | |||
| T2-T1 | –8.55 ± 2.70 | 0.69 ± 2.21 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


