Introduction
Because alveolar bone is used for skeletal anchorage, the variability and reliability of its dimensions are important.
Methods
Interradicular distances, cortical thicknesses, and buccolingual spaces were measured on computed tomography images of 22 adults (13 maxillary and 9 mandibular). Intra-arch analyses were done with paired t tests; the interarch comparisons were studied with independent t tests. The intraclass correlation coefficient was calculated between corresponding units.
Results
Interradicular distances were greater for the molars than for the incisors, and apical distances were greater than cervical. The mandibular lingual cortical thickness was the greatest, and the maxillary buccal cortical thickness was less than the mandibular in the molar apical zones. The widest and narrowest buccolingual spaces were found at the maxillary molars and the mandibular incisors, respectively. The cross values of cortical bone thickness were wider than the axial means and they had low agreement, so they had interradicular distances on the right and left sides.
Conclusions
Although interradicular distances must be carefully assessed, the molars were favorable sites for skeletal anchorage. Placing anchorage in anterior sites requires even more careful planning, including the use of computed tomography records.
The treatment goals of function, stability, and esthetics have not changed for decades, and the management of anchorage is still relevant to the quality of treatment outcomes. The required resistance to movement was mastered with biomechanics on a routine basis until the efficiency of skeletal anchorage was demonstrated. The application of orthodontic miniscrews and miniplates depends on the problem-oriented diagnosis and treatment-planning process. Based on adequate collection of data, emotional concerns should be seriously considered, and the conditions for fixation are described in detail. Of all the placement sites, the alveolar bone area demands the most reliable diagnosis.
The overall organization of the alveolar bone, along with the geometric complexity of multi-rooted teeth, is far more complex than bone diaphysis. There is anatomic variability between the regions of alveolar bone, implying certain limitations to standard fixation in narrow areas. If a normative arrangement of elements occurs in the alveolar areas, the advantages of a modified design in specific sites can be demonstrated for planning the mechanics, stability, and safety.
The evaluation of placement sites involves a systematic description of accessibility, conditions of the hard and soft tissues, availability of space, biomechanical application, irritation potential of the surrounding tissues, and patient comfort. The general possibilities for skeletal anchorage are determined when taking the patient’s medical history and in the clinical examination, whereas the protocol is established by analysis of diagnostic records regarding the alveolar dimensions. In addition to all possible sites of fixation, 3 dimensions have been given particular attention in the literature: cortical thickness, buccolingual space, and interradicular distance. These factors are important for selecting the miniscrew type as well as the angle and depth of placement. In areas with poor cortical bones, wide diameters and deep placements increase stability. However, the miniscrews should be smaller than the interradicular distance, and the depth of placement cannot exceed the buccolingual space. The appropriateness of a specific protocol of placement should be estimated from a comprehensive data set.
Computed tomography (CT) is a relatively new orthodontic diagnostic record that allows for detecting the 3-dimensional arrangement of anatomic elements with submillimetric resolution. The overall match between the microfocus CT and the histologic analysis of the trabecular bone is about 89%. Otherwise, the routine use of CT records is still not justified from the radiation-protection point of view. For this reason, it is interesting to answer these questions. When are CT records essential to skeletal anchorage? What is the reliability of measurements on CT? The objectives of this study were to evaluate the pattern of variability of the alveolar dimensions in the placement sites and to comprehend the reliability of the values measured on CT sections.
Material and methods
The sample comprised 22 adults (mean age, 37 ± 9 years) with complete permanent dentitions, periodontal health, and no history of systemic diseases. The maxillary arch was studied in 13 subjects (8 men, 5 women) and the mandibular arch in 9 (5 men, 4 women). A high-resolution CT image (Somaton Spirit, Siemens, Munich, Germany) was obtained for analysis of the dental arch where skeletal anchorage was planned. The thickness and the interval of axial sections were 1.0 and 1.0 mm, respectively, at the posterior region of arch. The CT image was reconstructed with Dental Slices software (version 2.1.1, Conexão, São Paulo, Brazil), and linear measurements were made in the axial, cross, and panoramic planes of view ( Fig 1 ).
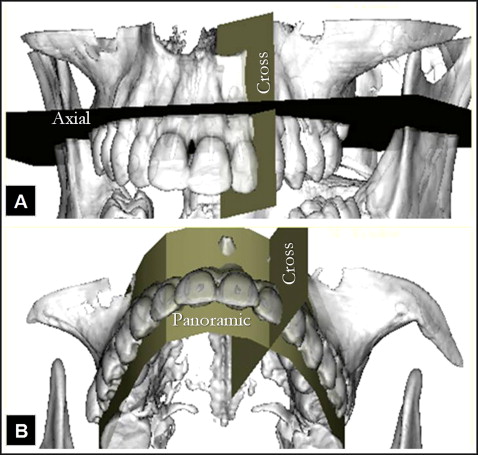
The original CT sections were obtained in the axial plane, which is orthogonal to the long axis of a patient’s head and parallel to the occlusal plane ( Fig 1 , A ). Perpendicularly to the axial plane, panoramic curves were drawn passing through the middle of the roots of the anterior teeth and the center of the buccal roots in the posterior areas ( Fig 1 , B ). The software generated the cross views with lines that were 32 mm long, perpendicular to the tangent of the panoramic curves ( Fig 1 ). By arranging the axial, panoramic, and cross views of the studied sites, a system of coordinates was obtained. In each view, there were indicator lines for locating the other 2 planes ( Fig 2 ).
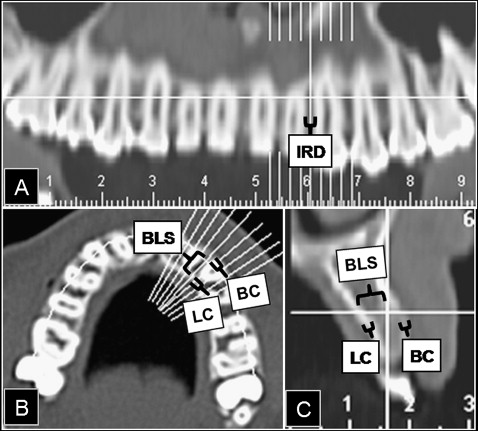
Interradicular distances, cortical thicknesses, and buccolingual spaces were measured on the right and left sides of the maxillary and mandibular arches. The mesiodistal distance between 2 adjacent roots represented the interradicular distance. This dimension was measured on the panoramic CT view ( Fig 2 , A ) by using the axial and cross indicator lines as references. Cortical thickness was defined as the width of the cortical bone; buccolingual space was the linear distance between the buccal and lingual cortical plates ( Fig 2 , B and C ). The cortical thicknesses and the buccolingual spaces were measured on the axial view considering the coordinates of the cross and panoramic indicators ( Fig 2 , B ). All 3 dimensions were measured in both cervical and apical zones. In addition to measuring cortical thicknesses and buccolingual spaces in the axial plane, we also studied the corresponding apical dimensions in the cross view ( Fig 2 , C ) to determine the reliability of the image sources. The cervical and apical vertical levels were located in the panoramic and cross views with the axial indicator line, when assessing the incisor and molar areas.
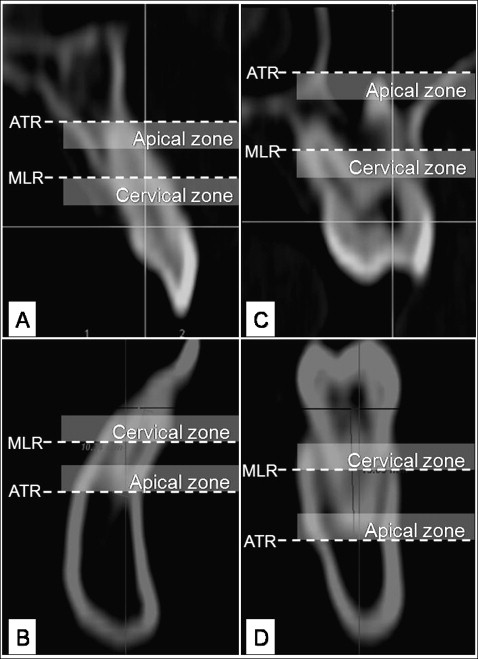
The incisor sites represented the area between the lateral incisors and the canines ( Fig 3 , A and B ); the molar sites comprised the region between the second premolars and the first molars ( Fig 3 , C and D ) bilaterally. The alveolar zones in the incisor sites were defined according to the root length of the lateral incisors, whereas the molar zones were classified according to the mesial roots of the first molars. The midpoint and the apical tip of these roots were identified, and the 2.0-mm area gingival to these landmarks comprised the cervical and apical zones, respectively ( Fig 3 ).
The measurements were repeated by the same operator (F.L.M.) on days 7 and 14 after the first event, and analysis of variance (ANOVA) ( P <0.05) was conducted. There were no statistically significant differences between the measurements, thus validating the method and allowing for the use of arithmetic means for repeated values.
Statistical analysis
Molar and incisor sites in the dental arch were compared by using the paired t test, and a t test for independent samples was applied for comparisons between the maxillary and mandibular sites. The apical and cervical zones were analyzed with a paired t test for interradicular distances and buccolingual spaces. Differences between the buccal and lingual cortical bones in the apical and cervical zones of single sites were calculated by pairwise comparisons with the Bonferroni adjustment.
The means of the differences between the axial and cross sections were determined, and the paired t test was used for comparing the measured sections. The reliability of the data was evaluated by calculating the intraclass correlation coefficient (ICC) between the axial and cross measurements for confidence of 95%. Accordingly, the axial values on the right and left sides of the arch were compared, and the analysis of reliability was carried out. Based on the clinical importance of measurement errors, the significance might be high (ICC ≥0.95), acceptable (0.80 >ICC <0.95), or low (ICC ≤0.80).
Results
In the maxillary and mandibular cervical zones, the interradicular distances of the molars were significantly greater than those of the incisor sites. The apical distance was statistically wider than the cervical one in the anterior areas ( Table I ). The mandibular lingual cortical bone was statistically thicker than in other places, even though, in the mandibular incisors, the cervical mean was less thick than the apical. The maxillary buccal cortical bone was less thick than the lingual one and the mandibular buccal cortical bone in the corresponding apical zones ( Table II ). The buccolingual spaces in the incisor sites were statistically narrower than the molar ones; the greatest width was found in the maxillary molars. For the maxillary incisors, the apical width was larger than the cervical mean ( Table III ).
| Maxillary arch (mean ± SD) | Mandibular arch (mean ± SD) | Maxillary x mandibular ( P value † ) | ||||||
|---|---|---|---|---|---|---|---|---|
| Apical | Cervical | P value ∗ | Apical | Cervical | P value ∗ | Apical | Cervical | |
| Molars | 2.4 ± 1.5 | 2.1 ± 1.2 | 0.115 | 2.3 ± 0.7 | 2.1 ± 0.5 | 0.111 | 0.457 | 0.457 |
| Incisors | 1.8 ± 0.5 | 1.4 ± 0.4 | 0.008 | 1.8 ± 0.4 | 1.4 ± 0.5 | 0.018 | 0.422 | 0.484 |
| P value ∗ | 0.218 | 0.017 | 0.061 | 0.008 | ||||
| Maxillary (mean ± SD) | Mandibular (mean ± SD) | Maxillary x mandibular ( P value ‡ ) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BCa | BCc | LCa | LCc | P value ∗ | BCa | BCc | LCa | LCc | P value ∗ | BCa | BCc | LCa | LCc | |
| Molars | 0.9 ± 0.05 | 1.0 ± 0.03 | 1.3 ± 0.05 | 1.2 ± 0.03 | 0.0001 | 1.3 ± 0.09 | 1.0 ± 0.05 | 2.0 ± 0.2 | 1.4 ± 0.07 | 0.0001 | 0.0001 | 0.068 | 0.0001 | 0.012 |
| Incisors | 0.9 ± 0.03 | 0.9 ± 0.02 | 1.3 ± 0.09 | 1.2 ± 0.03 | 0.0001 | 1.1 ± 0.06 | 0.9 ± 0.04 | 1.7 ± 0.12 | 1.4 ± 0.07 | 0.0001 | 0.0001 | 0.404 | 0.010 | 0.002 |
| P value † | 0.112 | 0.002 | 0.762 | 0.100 | 0.020 | 0.005 | 0.095 | 0.893 | ||||||
∗ Pairwise comparisons (Bonferroni adjustment) demonstrating differences: maxillary molars (LC >BC); mandibular molars (Lca >BC and LCc >BCc); maxillary incisors (LC >BC); mandibular incisors (LC >Bca >BCc).
| Maxillary (mean ± SD) | Mandibular (mean ± SD) | Maxillary x mandibular ( P value † ) | ||||||
|---|---|---|---|---|---|---|---|---|
| Apical | Cervical | P value ∗ | Apical | Cervical | P value ∗ | Apical | Cervical | |
| Molars | 8.7 ± 2.3 | 8.2 ± 1.6 | 0.142 | 7.0 ± 1.1 | 6.5 ± 0.9 | 0.125 | 0.016 | 0.005 |
| Incisors | 6.0 ± 2.0 | 5.1 ± 1.7 | 0.027 | 5.1 ± 1.2 | 4.9 ± 1.4 | 0.420 | 0.101 | 0.416 |
| P value ∗ | 0.001 | 0.0001 | 0.0001 | 0.005 | ||||
The differences in cortical thickness measured in the axial and cross planes demonstrated higher values on the cross sections. The buccal cortical and mandibular lingual bone thicknesses were statistically greater in the cross view than in the axial one. The ICC values between the axial and cross sources of measurement were acceptable for the lingual cortical thickness and low for buccal cortical bone. There was a high ICC between the axial and cross measurements of buccolingual space, although a significantly positive difference was found in the maxillary incisors ( Table IV ).
| Buccal cortical | Lingual cortical | Buccolingual space | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Difference (mean ± SD) | P value ∗ | ICC (alpha) | Difference (mean ± SD) | P value ∗ | ICC (alpha) | Difference (mean ± SD) | P value ∗ | ICC (alpha) | |
| Maxillary | |||||||||
| Molar | −0.06 ± 0.14 | 0.015 | .798 | −0.01 ± 0.15 | 0.398 | .883 | −0.01 ± 0.32 | 0.429 | .995 |
| Incisors | −0.08 ± 0.13 | 0.002 | .592 | −0.02 ± 0.18 | 0.253 | .893 | 0.15 ± 0.28 | 0.007 | .995 |
| Mandibular | |||||||||
| Molars | −0.24 ± 0.25 | 0.0004 | .765 | −0.22 ± 0.24 | 0.0006 | 0.933 | 0.06 ± 0.45 | 0.285 | .963 |
| Incisors | −0.10 ± 0.21 | 0.031 | .735 | −0.22 ± 0.22 | 9.0003 | 0.865 | 0.07 ± 0.31 | 0.167 | .986 |
In the maxillary arch, the right and left sides were highly correlated for interradicular distance and buccolingual space. In contrast, a low ICC was found for mandibular interradicular distances and maxillary buccal cortical bone. In addition, the mandibular lingual cortical bone in the incisor apical zones and the maxillary buccolingual space in the molar cervical sites were statistically greater on the right than on the left side of the arch. These statistical differences between sides were found along with an acceptable level of ICC ( Table V ).


