Introduction
Study models are an essential part of an orthodontic record. Digital models are now available. One option for generating a digital model is cone-beam computed tomography (CBCT) scanning of orthodontic impressions and bite registrations. However, the accuracy of digital measurements from models generated by this method has yet to be thoroughly evaluated.
Methods
A plastic typodont was modified with reference points for standardized intra-arch and interarch measurements, and 16 sets of maxillary and mandibular vinylpolysiloxane and alginate impressions were made. A copper wax-bite registration was made with the typodont in maximum intercuspal position to accompany each set of impressions. The impressions were shipped to OrthoProofUSA (Albuquerque, NM), where digital orthodontic models were generated via CBCT. Intra-arch and interarch measurements were made directly on the typodont with electronic digital calipers and on the digital models by using OrthoProofUSA’s proprietary DigiModel software.
Results
Percentage differences from the typodont of all intra-arch measurements in the alginate and vinylpolysiloxane groups were low, from 0.1% to 0.7%. Statistical analysis of the intra-arch percentage differences from the typodont of the alginate and vinylpolysiloxane groups had a statistically significant difference between the groups only for maxillary intermolar width. However, because of the small percentage differences, this was not considered clinically significant for orthodontic measurements. Percentage differences from the typodont of all interarch measurements in the alginate and vinylpolysiloxane groups were much higher, from 3.3% to 10.7%. Statistical analysis of the interarch percentage differences from the typodont of the alginate and vinylpolysiloxane groups showed statistically significant differences between the groups in both the maxillary right canine to mandibular right canine (alginate with a lower percentage difference than vinylpolysiloxane) and the maxillary left second molar to mandibular left second molar (alginate with a greater percentage difference than vinylpolysiloxane) segments. This difference, ranging from 0.24 to 0.72 mm, is clinically significant.
Conclusions
In this study, digital orthodontic models from CBCT scans of alginate and vinylpolysiloxane impressions provided a dimensionally accurate representation of intra-arch relationships for orthodontic evaluation. However, the use of copper wax-bite registrations in this CBCT-based process did not result in an accurate digital representation of interarch relationships.
Accurate records are essential for effective orthodontic diagnostic and treatment planning. Historically, this need was satisfied by 2-dimensional and 3-dimensional (3D) representations of the patient’s craniofacial anatomy, of which study models were the only 3D component. Although plaster models have a few drawbacks, including required laboratory processing time, need for supporting material inventory, potential breakage, and space for storage, confidence in their accuracy has not been one of them. Plaster models continue to be the gold standard for orthodontic diagnosis, discussions with patients and colleagues, treatment progress evaluation, and treatment documentation. Additionally, plaster models are commonly preferred by orthodontists for their ease of manipulation in ascertaining the degree of decompensation required for surgical treatment, the transverse relationships associated with proposed sagittal changes, the extraction pattern possibilities, and the details of tooth morphology.
The potential clinical and logistic advantages of digital orthodontic models have been published previously, including reduced need for physical storage space, increased ease of portability, and maintenance of model integrity and quality. Current research has also shown comparable accuracy of linear measurements made on digital models with those on plaster models, demonstrating their validity as an alternative for diagnostic analysis and treatment planning, and their suitability for occlusal measurements with the peer assessment rating index. Although some reports show promise concerning possible submission of digital models to the American Board of Orthodontics, to date, computerized scoring with the its objective grading system has yet to be proven comparable with manual grading by using currently available software. Additional applications for digital models continue to be discovered; the literature describes their integration with existing 3D imaging technologies such as cone-beam computed tomography (CBCT) and 3D photography, demonstrating the potential for a true 3D reconstruction of the patient’s craniofacial complex for orthodontic diagnosis, treatment planning, progress assessment, and documentation.
Currently, there are 3 methods of producing digital orthodontic study models by 7 companies.
- 1.
Laser scanning of plaster models (OrthoCAD by Cadent, Carlstadt, NJ; emodels by Geodigm, Chanhassen, Minn; ortho·graphics by Ortho Cast, High Bridge, NJ; Ortho Insight 3D by Innovative Software Design, Chattanooga, Tenn).
- 2.
CBCT imaging of orthodontic impressions or plaster models (DigiModel by OrthoProofUSA, Albuquerque, NM; Invisalign by Align Technologies, Santa Clara, Calif).
- 3.
Direct, intraoral laser scanning of the dental arches or in-office scanning of plaster models (OrthoCAD by Cadent; SureSmile by Orametrix, Richardson, Tex).
Although laser surface scanning of plaster models generated from alginate or vinylpolysiloxane impressions has been studied extensively, with a comparable level of accuracy to plaster models, the more-recently developed method of CBCT scanning of alginate impressions has not yet received as extensive an examination. Although this method is comparable with the scanning process used by Invisalign for vinylpolysiloxane impressions, because of the costs involved, most practitioners prefer to use a material that has less dimensional stability over time. Therefore, although this process is promising, requiring no intermediate plaster models, the accuracy of the entire process from alginate impression to final digital model set has not been thoroughly tested.
Like the systems that use laser surface scanning of plaster models, OrthoProofUSA requires 2-day shipping of the alginate impressions and associated bite registration to the company for processing. The scanning process is completed by using Hytec’s (subsidiary of IMTEC, Ardmore, Okla) proprietary FlashCT technology to create digital models directly from the alginate impressions and bite registration. Since this process eliminates the need to pour the impression, the belief is that any errors in that process would be eliminated and accuracy improved. To optimize the accuracy of the process, OrthoProofUSA recommends using either a 100-hour dimensionally stable alginate or vinylpolysiloxane for orthodontic impressions.
Therefore, this study was undertaken to answer 2 questions. How do intra-arch measurements of digital models from CBCT scanning of 100-hour stable alginate impressions compare with those from vinylpolysiloxane impressions when shipped under the same conditions? Does the use of a copper wax-bite registration result in an accurate reproduction of interarch dimensions, when used to generate digital model sets in this CBCT-based system? The null hypothesis was that the percentage differences, in reference to a standardized model set, between the interarch and intra-arch measurements on digital models from vinylpolysiloxane (Aquasil, Dentsply Caulk, York, Pa) and those from 100-hour stable Kromopan 100 (Kromopan USA, Morton Grove, Ill) alginate impressions would not be statistically significant.
Material and methods
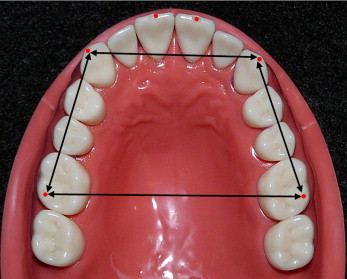
A plastic typodont (D91SDP-500B.1, Kilgore International, Inc, Coldwater, Mich) was modified to allow accurate intra-arch and interarch measurements. The typodont was scored with a number 2 round bur in the locations marked in red in Figure 1 to allow consistent measurements between points.

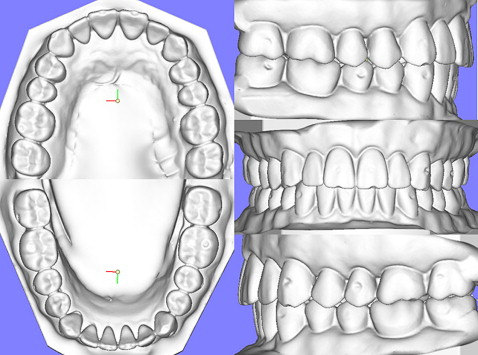
OrthoProofUSA and Kromopan USA differ in their recommendations for shipping alginate impressions. When the alginate impressions are not poured immediately, Kromopan USA recommends sealing them in a plastic bag with no additional materials. OrthoProofUSA recommends wrapping the impressions in moist paper towels before sealing them in a plastic bag. Because of the different recommendations, a pilot study was conducted to analyze whether these 2 methods would result in a statistically significant difference between measurements on the digital models. Five impressions each of vinylpolysiloxane, Kromopan 100 with a paper towel, and Kromopan 100 without a paper towel were made of the typodont maxillary arch. The 15 impressions were boxed and shipped to OrthoProofUSA via FedEx 2-day shipping per company instructions. OrthoProofUSA contacted the primary investigator (A.J.W.) on receipt of all impressions, when they were scanned sequentially. Transverse and anteroposterior measurements (intercanine, intermolar, canine-molar right, canine-molar left), shown in Figure 2 , were completed on the digital models for comparison.
Additionally, the pilot study allowed the primary investigator to become proficient in obtaining consistently accurate measurements and using the digital caliper and DigiModel software before the main study.
Sixteen sets each of vinylpolysiloxane and alginate maxillary and mandibular impressions were made of the typodont. For the vinylpolysiloxane impressions, Caulk tray adhesive (Dentsply Caulk) was painted in plastic impression trays provided by OrthoProofUSA and allowed to dry. Each tray was customized by placing Aquasil EasyMix vinylpolysiloxane putty (Dentsply Caulk) in the tray with a polyethylene spacer to provide space for the wash impression and then seated on the typodont. After the putty set, the polyethylene spacer was removed from the customized trays, and Aquasil Smart Wetting monophase vinylpolysiloxane (Dentsply Caulk) wash impressions were made of the typodont. The impressions were sealed in individual plastic bags as recommended by OrthoProofUSA.
For the alginate impressions, liquid tray adhesive (Hold, Waterpik Technologies, Newport Beach, Calif) was sprayed in plastic impression trays from OrthoProofUSA and allowed to dry. Kromopan 100 alginate was vacuum mixed (300250, Jelenko, San Diego, Calif), and impressions were made of the typodont according to the manufacturer’s instructions. The impressions were rinsed with water, wrapped in moist paper towels, and immediately sealed in individual plastic bags as recommended by OrthoProofUSA.
For each set of impressions, a copper wax-bite registration (Surgident, Heraeus Kulzer, South Bend, Ind) was made with the typodont in maximum intercuspal position as recommended by OrthoProofUSA. The bite registrations were placed in individual hard plastic containers (provided by OrthoProofUSA) to prevent distortion during shipping. The 32 sets of impressions and bite registrations were boxed and shipped to OrthoProofUSA via 2-day shipping per company instructions. OrthoProofUSA contacted the primary investigator on receipt of all impressions, when they were scanned sequentially. The average time between making the impressions and their CBCT scanning was 47.5 hours. The vinylpolysiloxane models served as the transport control with which the alginate models were compared.
The data were collected from measurements in 3 categories ( Figs 2-4 ).
- 1.
Arch perimeter was measured by a modified segment arch method. Segment A was the distance from the bur mark on the right first permanent molar to the mark on the right canine. Segment B was the distance from the mark on the right canine to the mark on the right central incisor. Segment C was the distance from the mark on the right central incisor to the mark on the left central incisor. Segment D was the distance from the mark on the left central incisor to the mark on the left canine. Segment E was the distance from the mark on the left canine to the mark on the left first permanent molar. The segments were summed to the nearest 0.1 mm to equal the arch perimeter for both arches.
- 2.
Arch width. Intermolar width was measured as the distance between the occlusal bur marks on the first permanent molars. Intercanine width was measured as the distance between the incisal bur marks on the permanent canines. These measurements were made on both maxillary and mandibular models. Measurements were recorded to the nearest 0.1 mm.
- 3.
Interarch measurements were made with the typodont and digital models occluded to assess the accuracy of the bite registration in reproducing the relationships of the arches in occlusion. The measurements were made from the buccal or labial bur mark on each maxillary tooth to the buccal or labial bur mark on the corresponding mandibular tooth (ie, maxillary right second molar to mandibular right second molar, maxillary right first premolar to mandibular right first premolar, and so on). Measurements were recorded to the nearest 0.1 mm.

Electronic digital calipers (Fowler/NSK PRO-MAX, Fred V. Fowler, Newton, Mass) were used to measure the typodont. OrthoProofUSA’s DigiModel software (version 2.3.5, build 8) with an optical computer mouse was used to make the measurements on the digital models. The monitor used was a 17-in LCD (Dell, Inc, Round Rock, Tex) with a resolution of 1280 × 1024 pixels and 32-bit color. All measurements were made 3 times to the nearest 0.1 mm, and means and standard deviations were calculated.
The digital measurements were subtracted from the typodont measurements, and an absolute difference was obtained. The percentage change from the typodont was determined for each digital measurement, and the mean and standard deviation determined. The intra-arch data were analyzed with 2-way analysis of variance (ANOVA) to evaluate the effects of impression material (2 levels) and segmental measurement (3 levels) on percentage differences from the typodont for both arches (α = 0.05). The interarch data were analyzed with 2-way ANOVA to evaluate the effects of impression material (2 levels) and segmental measurement (8 levels) on the percentage differences from the typodont (α = 0.05). The Tukey post-hoc test was used to compare pairwise differences between mean values. Additionally, unpaired t tests were used per segmental measurement to compare the percentage differences between impression materials. The Bonferonni adjustment with an alpha level of 0.01 was applied as a multiple-comparison correction when several statistical tests were performed simultaneously.
Results
The pilot study showed, with 1-way ANOVA, no statistically significant differences between the intra-arch measurements in any group ( P >0.05). Therefore, the alginate submission recommendations of OrthoProofUSA were followed for the main study. Additionally, the primary investigator’s ability to record consistently accurate measurements using the digital calipers and DigiModel software was demonstrated by the extremely small variability of the repeated measurements.
Statistical analysis of the intra-arch measurements showed findings specific for each arch. For the maxillary intra-arch measurements, 2-way ANOVA found a significant difference in the percentage difference from the typodont based on impression material ( P <0.001) or segmental measurement ( P <0.001), but there was a significant interaction ( P <0.001). Unpaired t tests found no significant difference between the 2 impression materials for arch perimeter and intercanine measurements but showed a significant difference for intermolar measurements. For the intermolar measurements, the alginate material resulted in a significantly smaller percentage difference from the typodont than did the vinylpolysiloxane material ( Table I ). For the mandibular intra-arch measurements, 2-way ANOVA found no significant difference in the percentage difference from the typodont based on impression material ( P = 0.124) but a significant difference based on segmental measurement ( P <0.001), with no significant interaction ( P = 0.951) ( Table II ). For the interarch measurements, 2-way ANOVA found a significant difference in percentage difference from the typodont based on impression material ( P = 0.001) and segmental measurements ( P <0.001), but there was a significant interaction ( P <0.001). Unpaired t tests found no significant difference between the 2 impression materials except for the maxillary right canine to mandibular right canine and the maxillary left second molar to mandibular left second molar segmental measurements ( Table III ).
| Impression material | Arch perimeter | Intercanine width | Intermolar width |
|---|---|---|---|
| Alginate | 0.1 (0.1) | 0.3 (0.2) | 0.2 (0.2) ∗ |
| Vinylpolysiloxane | 0.2 (0.2) | 0.3 (0.2) | 0.6 (0.6) ∗ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


