Introduction
An accurate prediction of the mesiodistal diameter (MDD) of the erupting permanent teeth is essential in orthodontic diagnosis and treatment planning during the mixed dentition period. Our objective was to test the accuracy and reproducibility of cone-beam computed tomography (CBCT) in predicting the MDD of unerupted teeth. Our secondary objective was to determine the accuracy and reproducibility of 3 viewing methods by using 2 CBCT software programs, InVivoDental (version 4.0; Anatomage, San Jose, Calif) and CBWorks (version 3.0, CyberMed, Seoul, Korea) in measuring the MDD of teeth in models simulating unerupted teeth.
Methods
CBCT data were collected on the CB MercuRay (Hitachi Medical Corporation, Tokyo, Japan). Models of unerupted teeth (n = 25), created by embedding 25 tooth samples into a polydimethylsiloxane polymer with a similar density to tissues surrounding teeth, were scanned and measured by 2 investigators. Repeated MDD measurements of each sample were made by using 3 CBCT viewing methods: InVivo Section, InVivo Volume Render (both Anatomage), and CBWorks Volume Render (version 3.0, CyberMed). These measurements were then compared with the MDD physically measured by digital calipers before the teeth were embedded and scanned.
Results
All 3 of the new methods had mean measurements that were statistically significantly less ( P <0.0001) than the physical method, adjusting for investigator and tooth effects. Specifically, InVivo Section measurements were 0.3 mm (95% CI, −0.4 to −0.2) less than the measurements with calipers, InVivo Volume Render measurements were 0.5 mm less (95% CI, −0.6 to −0.4) than those with calipers, and CBWorks Volume Render measurements were 0.4 mm less (95% CI, −0.4 to −0.3) than those with calipers.
Conclusions
Overall, there were high correlation values among the 3 viewing methods, indicating that CBCT can be used to measure the MDD of unerupted teeth. The InVivo Section method had the greatest correlation with the calipers.
An essential factor in orthodontic diagnosis and treatment planning is the ability to predict the size of unerupted teeth during the mixed dentition period. An accurate prediction of the mesiodistal diameter (MDD) of the erupting permanent teeth will help to determine whether there will be sufficient space for the permanent teeth to erupt unimpeded and properly aligned in their respective arches. In particular, it is necessary to predict the MDD of the crowns of the unerupted canines and premolars (C, P1, and P2). A previous study comparing the MDD of deciduous canines and molars to their permanent successors found that permanent canines are significantly broader and permanent premolars are smaller than their predecessors. Overall, the sum of the crown widths of these permanent teeth has been reported to be lower than that of their deciduous predecessors. A discrepancy between the space required for the dentition and the space available in the dental arch will result in excessive spacing or crowding. Hence, an accurate estimate of the sum of crown widths vs available space is necessary for making competent decisions concerning eruption guidance, serial extractions, space maintenance, space regaining, and other options in orthodontic treatment planning.
Different methods for estimating the sizes of unerupted teeth have been developed. In the literature, 4 groups of methods are commonly used to predict the MDD of the permanent C, P1, and P2 before eruption: analyses based on mean values of the C, P1, and P2 by using established tables of average tooth sizes ; regression equations based on high linear correlations between relevant groups of teeth ; measurements of the unerupted teeth taken directly from radiographs ; and analyses with a combination of regression equations and radiographic methods.
Numerous studies have been conducted to compare the accuracy of various methods of predicting the MDD of the C, P1, and P2. Despite the diversity and numbers of available methods, no single method has been shown to deliver high accuracy, precision, and reliability; all have limitations. For example, a study comparing 8 commonly used regression methods found that prediction methods either overestimated (Legovic and Hautz, Droschl et al, Tanaka and Johnston, and Moyers ) or underestimated (Bachmann, Trankmann et al, and Gross and Hasund ) the sums of crown widths of the C, P1, and P2. Gardner compared 4 methods (Nance, Tanaka and Johnston, Moyers, and Hixon and Oldfather ) and also found that the methods either overestimated or underestimated the crown widths of the canines and the premolars. Another significant limitation of existing regression methods is their inability to be applied universally when variations occur between populations. Some methods are less reliable for female patients, raising the question of sex variations.
There is a clear need for a highly accurate and reliable method for predicting the crown widths of unerupted permanent canines and premolars for orthodontic purposes. In this study, we examined whether a significant diagnostic advancement in clinical diagnosis, cone-beam computed tomography (CBCT), can be used to provide accurate and reliable measurements of simulated unerupted teeth. We hypothesized that images from CBCT will provide accurate and reliable linear measurements of MDD and eliminate limitations based on individual variations. Support for this hypothesis is provided by the following factors.
- 1.
CBCT allows an area of interest to be observed from many angles.
- 2.
In addition to advanced image reconstruction algorithms, the subject can be reconstructed in 3 dimensions at high resolution. These images are precise in locating and measuring the desired details.
- 3.
Few studies have shown distortion and errors across the scan volumes produced by CBCT.
- 4.
Furthermore, a study indicated that segmented volumes of craniofacial structures from CBCT data are accurate model representations of the objects with respect to linear measurements.
Numerous studies have been performed to assess the applications and benefits of CBCT (including treatment planning in dental implant and airway studies ). Although the accuracy and reliability of linear dental measurements on CBCT have been well assessed, no one, to the best of our knowledge, has studied the accuracy and reliability of CBCT in predicting the size of unerupted teeth. The primary aim of this study was to investigate the accuracy of the MDD of the C, P1, and P2 measured by using CBCT scans compared with physical measurements from digital calipers, which is the current gold standard.
Our secondary aim was to compare the accuracy and reproducibility of 2 CBCT software programs, InVivoDental and CBWorks (version 3.0; CyberMed, Seoul, Korea), in measuring the MDD of teeth in models simulating unerupted teeth.
Material and methods
Twenty-five extracted teeth (11 premolars, 14 molars) were selected. Two investigators (E.N. and M.O.) first measured each tooth’s MDD using digital calipers (Mitutoyo Canada, Toronto, Ontario, Canada) with a nominal resolution of ±0.01 mm. The measurement with calipers is a physical measurement and was considered the gold standard for the purpose of this study. Each investigator recorded measurements made at 3 times to allow calculation of arithmetic means and associated errors. The measurement sessions were 1 week apart.
All 25 teeth were embedded in Aquasil Easy Mix Putty (Dentsply, Des Plaines, Ill), simulating the supporting structures of the teeth in the dental arches. Aquasil is a hydrophilic addition-reaction silicone impression material composed of polydimethylsiloxane polymer, calcium sulfate, silicon dioxide, polymethylhydrogen siloxane, surfactant, plasticizer, and pigments. It has a density of 250 to 600 Hounsfield units (HU); this is similar to the density of the supporting dental tissues (bone and soft tissues, 200-700 HU). Tooth enamel, with a density of approximately 2100 to 4000 HU, can be easily discriminated from the surrounding tissues in the CBCT images. The rigidity of Aquasil allowed for retention of the teeth and prevented movement.
The dental arch models were scanned by using the CB MercuRay (Hitachi Medical Corporation, Tokyo, Japan) in the Division of Orthodontics, School of Dentistry, at the University of California at San Francisco. The scanning parameters used were 110 kVp, 2 mA, 9.6 seconds per revolution, and a 12-in field of view. The voxel size of the CB MercuRay scanner with these settings is 0.4 mm, and the physical spatial resolution is 0.7 mm. The volumetric data were then analyzed with the 2 CBCT software programs, InVivoDental and CBWorks. Two measurement methods were used with the InVivo Dental software and 1 method with CBWorks, each described below. Two investigators measured 25 teeth at 3 times using each of the 4 methods: physical measurement, InVivo Section, InVivo Volume Render, and CBWorks Volume Render.
With InVivoDental, 2 analyzing modes were used as methods of measuring the MDD of the embedded teeth: the Section mode and the Volume Render mode.
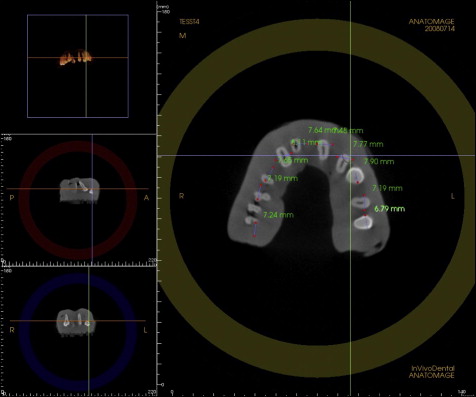
In the InVivo Section mode, the x, y, and z sections (axial, coronal, sagittal) were combined simultaneously for 2-dimensional visualization. A 3-dimensional (3D) volume visualization was displayed on the same screen as the 2-dimensional visualization. In this mode, the scalar value of selected voxels is displayed in Hounsfield units; this allows soft tissue to be distinguished from enamel when taking measurements with the “Distance” tool. By using the 2-dimensional and 3D visualizations simultaneously, the image of each tooth of interest was oriented perpendicular to the occlusal plane to allow the largest MDD to be visualized and measured (with measurements recorded to the nearest 0.1 mm) ( Fig 1 ).
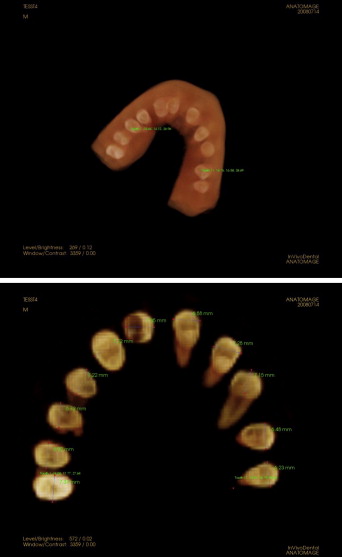
With the InVivo Volume Render mode, it is possible for the scanned region to be reconstructed 3 dimensionally. This mode has presets that allow for the display of structures according to their specified densities. For this study, it was determined that the “Bone” and “Teeth” presets would be used because they allowed visualization of the hard tissues (embedded teeth) but prevented visualization of the surrounding impression material. We then used the “Sculpting” tool in the Volume Render mode to allow the image of each tooth requiring measurement to be segregated from the surrounding tissues and adjacent teeth. Finally, the “Measure 3D Distance” tool in the software was used to measure the MDD from the 3D image, with measurements recorded to the nearest 0.1 mm ( Fig 2 ).
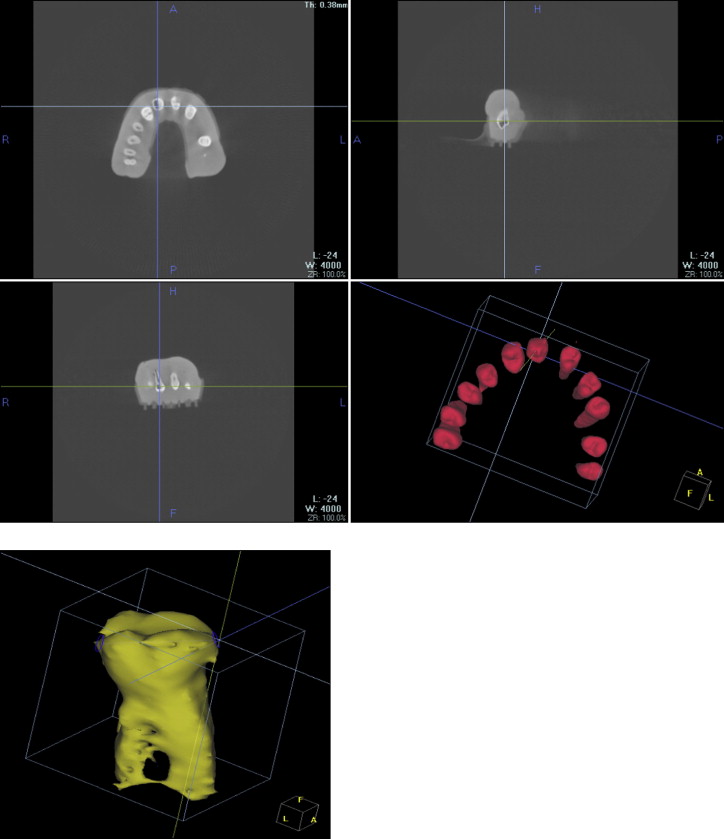
In CBWorks, the Volume Render mode was used to measure the MDD in this study. This mode creates a 3D image (volume-rendering image) from the volumetric data. A histogram in CBWorks’ on-screen control panel was used to adjust the images for optimal opacity. Similar to InVivo, each tooth of interest was then “sculpted out” for individual display with the “Sculpt” tool, and MDD measurements for each tooth were recorded to the nearest 0.1 mm with the “Measuring” tool ( Fig 3 ).
Results
For each of the 3 CBCT methods and the physical method, the reproducibility of all measurements was first determined. For each investigator and each method, data were analyzed by using 1-way analysis of variance (ANOVA) with tooth as the fixed effect. The intraclass correlation (ICC) was also calculated. The ICC values ranged from 0 to 1. Values close to 1 indicate strong evidence of reproducibility. The results are displayed in Table I . For both 2 users, all 4 methods yielded an ICC greater than 0.95, indicating high reproducibility for any user of any of the 4 methods.
| Method | Investigator | ICC |
|---|---|---|
| InVivo Section | 1 | 0.98 |
| InVivo Volume Render | 1 | 0.98 |
| CBWorks Volume Render | 1 | 0.95 |
| Physical (calipers) | 1 | 0.99 |
| InVivo Section | 2 | 0.98 |
| InVivo Volume Render | 2 | 0.98 |
| CBWorks Volume Render | 2 | 0.97 |
| Physical (calipers) | 2 | 1.00 |
We then determined the reproducibility (or agreement) of values recorded by each investigator for each CBCT method and the physical method. An arithmetic mean of the 3 measurements made by each investigator on each tooth using each method was calculated. Then, the correlation coefficient (r) comparing the means of the 2 investigators for each method was determined. A correlation coefficient can range from 0 (no agreement) to 1 (perfect agreement). Of the 3 CBCT methods, the greatest agreement was obtained with the CBWorks Volume Render method, with a correlation of 0.97 (95% CI, 0.94 to 0.99), and the least agreement with the InVivo Volume Render method, with a correlation of 0.91 (95% CI, 0.80 to 0.96). The results are shown in Table II .
| Investigator 1 | Investigator 2 | n | Pearson correlation | Pearson 95% CI lower | Pearson 95% CI upper | Pearson P value |
|---|---|---|---|---|---|---|
| InVivo Section view method | ||||||
| Mean, measure 1 | Mean, measure 2 | 25 | 0.96 | 0.92 | 0.98 | <0.0001 |
| InVivo Volume Render method | ||||||
| Mean, measure 1 | Mean, measure 2 | 25 | 0.91 | 0.80 | 0.96 | <0.0001 |
| CBWorks Volume Render method | ||||||
| Mean, measure 1 | Mean, measure 2 | 25 | 0.97 | 0.94 | 0.99 | <0.0001 |
| Physical method (calipers) | ||||||
| Mean, measure 1 | Mean, measure 2 | 25 | 0.99 | 0.98 | 1.00 | <0.0001 |
The third goal was to determine the discrepancies between the measurements taken with each of the 3 CBCT methods and the physical method. An arithmetic mean of the 6 measurements taken by the 2 investigators for each tooth using each of the 3 CBCT methods was calculated. Correlation coefficients, relating the mean value for each CBCT method to the mean value for the physical method, were then determined. The InVivo Section method had the highest correlation (0.98) with the physical method. The results are displayed in Table III .
| IVar | JVar | n | Pearson correlation | Pearson 95% CI lower | Pearson 95% CI upper | Pearson P value |
|---|---|---|---|---|---|---|
| Physical | CBWorks Volume Render | 25 | 0.94 | 0.87 | 0.97 | <0.0001 |
| Physical | InVivo Sections view | 25 | 0.98 | 0.96 | 0.99 | <0.0001 |
| Physical | InVivo Volume Render | 25 | 0.97 | 0.93 | 0.99 | <0.0001 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


