An interdisciplinary approach is often the best option for achieving a predictable outcome for an adult patient with complex clinical problems. This case report demonstrates the combined periodontal/orthodontic treatment for a 49-year-old woman presenting with a Class II Division 1 malocclusion with moderate maxillary anterior crowding, a 9-mm overjet, and moderate to severe bone loss as the main characteristics of the periodontal disease. The orthodontic treatment included 2 maxillary first premolar extractions through forced extrusion. Active orthodontic treatment was completed in 30 months. The treatment outcomes, including the periodontal condition, were stable 17 months after active orthodontic treatment. The advantages of this interdisciplinary approach are discussed. Periodontally compromised orthodontic patients can be satisfactorily treated, achieving most of the conventional orthodontic goals, if a combined orthodontic/periodontic approach is used.
Orthodontic treatment is no longer a contraindication in the therapy of severe adult periodontal disease or in the maintenance of a healthy periodontium. In fact, orthodontic treatment could enhance the possibility of saving and restoring a deteriorated dentition.
Advanced periodontal disease is primarily characterized as severe attachment loss and a reduction of alveolar bone support, and the periodontal condition is usually characterized by tooth mobility, migration, spacing, and marginal gingival recession. In the maxillary anterior region, functional discomfort is usually accompanied by compromised esthetics. Orthodontic treatment for realignment of migrated periodontally involved teeth is initiated only after control of the periodontal inflammation has been achieved. If the patient is reasonably motivated and responds well to the initial periodontal therapy, adult orthodontic treatment has a role in providing complete rehabilitation in terms of both function and appearance, with a satisfactory long-term prognosis. Good oral hygiene at home and professional maintenance visits are important during and after active orthodontic treatment. In this periodontally compromised case, a successful result was achieved with improvement of oral hygiene, periodontal prognosis, esthetics, masticatory function, and self-confidence. This case report presents a modified (unusual) periodontal-orthodontic approach in an adult woman presenting with a Class II, Division 1 malocclusion with advanced periodontal disease (horizontal and vertical loss of alveolar bone), in whom 2 first maxillary premolar extractions were performed after forced extrusion. Both maxillary central incisors were also extruded to correct the bone and gingival levels, providing better esthetics and function.
Introduction
Diagnosis and etiology
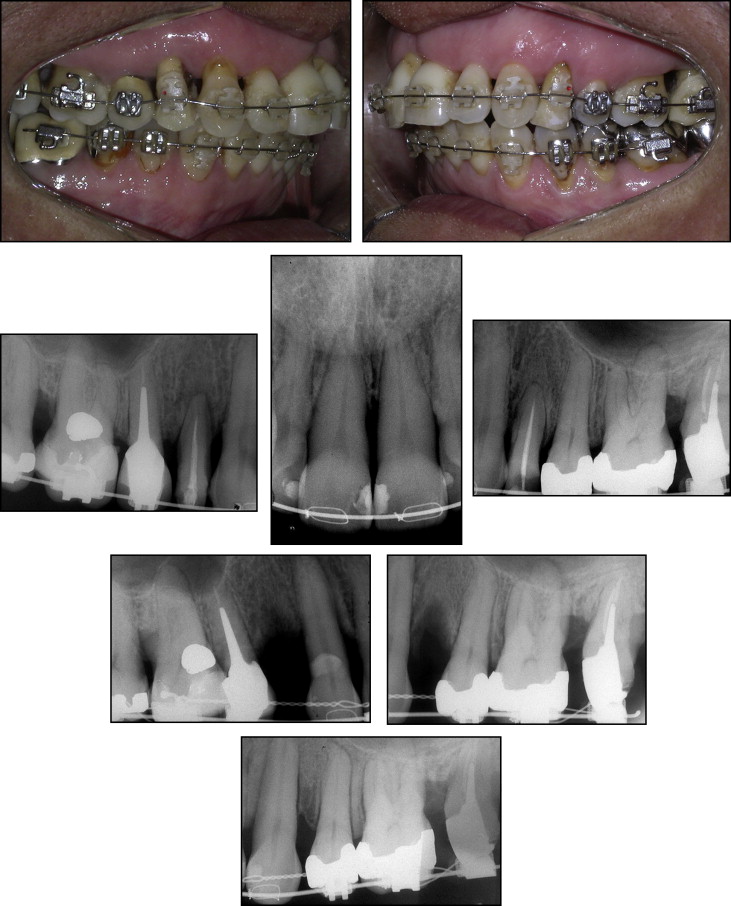
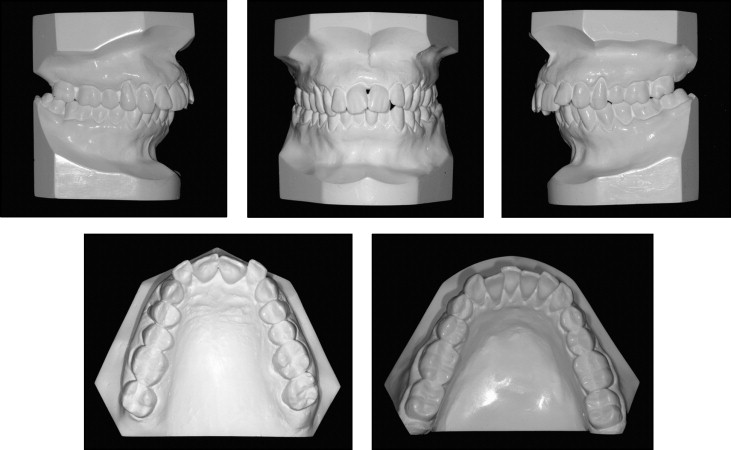
A 49 year-old female patient with severe periodontal disease, came to the private orthodontic office of one of us (M.J.), with the chief complaint about her maxillary anterior dental appearance. She had no systemic problems. The initial examination demonstrated an acute nasolabial angle and a strained lip closure. Significant gingival recession was noted labial to both maxillary first premolars, the maxillary and mandibular left molars, and the maxillary anterior segment (caused by previous periodontal surgery [resection]), with an open gingival embrasure ( Fig 1 ) between the central incisors. A furcation defect was present on the buccal surface of the mandibular left first molar. A complete Class II molar relationship on both sides, with severe maxillary protrusion and an overjet of 9 mm was identified. The maxillary and mandibular incisors were crowded, with mild migration and moderate rotation ( Fig 2 ).

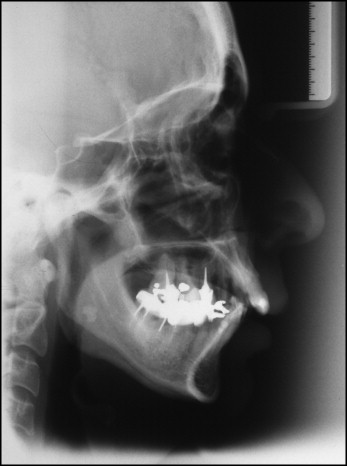
Probing of the periodontal attachment has been and still is the gold standard for diagnosis of active disease or progression of disease. Pretreatment periodontal probing demonstrated depths ranging from 3 to 8 mm, except for the maxillary lateral incisors and canines and the mandibular canines. Examination of radiographs taken before periodontal treatment demonstrated generalized horizontal bone loss in both arches and vertical bone defects in the maxillary first premolars and in the maxillary and mandibular second molars ( Fig 3 ). The cephalometric analysis showed a skeletal Class II jaw base relationship (ANB angle, 7.4°), with mandibular retrusion (SNB angle, 71.3°), a convex skeletal profile (NAP angle: 13.7°), a dolichofacial pattern with an increased SN-GoGn angle (41.6°), and protruded and labially tipped mandibular incisors ( Table I , Fig 4 ).

| 49 y 03 mo 8/4/04 | 52 y 07 mo 5/25/07 | |
|---|---|---|
| Variables | Pretreatment | Posttreatment |
| Maxillary Component | ||
| SNA angle (°) | 78.8 | 78.3 |
| A-Nperp (mm) | − 1.8 | −1.5 |
| Mandibular Component | ||
| SNB angle (°) | 71.3 | 70.1 |
| Pog-Nperp (mm) | −17.1 | −18.4 |
| Maxillomandibular Relationship | ||
| ANB angle (°) | 7.4 | 8.2 |
| Wits appraisal (mm) | 9.3 | 6.4 |
| Growth Pattern | ||
| FMA angle (°) | 30.6 | 31.4 |
| SN.OP (°) | 19.0 | 22.6 |
| SN.GOGN (°) | 41.6 | 42.6 |
| Facial Axis (°) | 78.7 | 77.4 |
| Lower anterior facial height (LAFH) (mm) | 72.6 | 75.2 |
| Profile | ||
| Convexity (°) | 13.7 | 14.6 |
| NL Angle (°) | 99.3 | 101.5 |
| Dentoalveolar Component | ||
| Upper 1 to NA (°) | 20.0 | 7.3 |
| Upper 1 to NA (mm) | 5.8 | −0.1 |
| Lower 1 to NB (°) | 31.8 | 37.0 |
| Lower 1 to NB (mm) | 8.3 | 10.1 |
| Lower 1 to MP (°) | 96.6 | 103.1 |
| Dental Relationships | ||
| Interincisal (°) | 117.3 | 123.8 |
| Overjet (mm) | 9.0 | 1.6 |
| Overbite (mm) | 4.1 | 1.7 |
Treatment objectives
The main objectives were to reduce or keep the defects at the same level, eliminate primary and secondary occlusal trauma by providing a functional occlusion and fixed retention between the teeth with bone loss, reduce the maxillary incisor protrusion, achieve an ideal overjet and overbite, and achieve satisfactory facial esthetics. It was also desirable to eliminate crowding and to correct the mesial inclination of the mandibular molars.
Treatment alternatives
One of the treatment options was to align the teeth without extractions, reducing the vertical defects of the maxillary premolars and the coronal height of central incisors by selective forced eruption and to perform interproximal enamel reduction in the maxillary arch to reduce the overjet. This option, although not ideal, would be more conservative, decreasing the root resorption risk of the anterior teeth.
The second option was extraction of the maxillary first premolars, but only after both teeth were forced to gradually extrude (“slow extraction”), inducing bone and gingival apposition and remodeling of the alveolar ridges. Subsequently, maxillary protrusion would be reduced. Endodontic root treatment, as well as extraction of the maxillary first premolars, would be the biological and additional cost of this alternative. This slow, forced eruption would also be applied to the maxillary central incisors to obtain a better crown-root proportion and to re-establish anterior esthetics with proper crown height.
The last treatment option was to reduce maxillary protrusion with orthognatic surgery and to reduce the periodontal pockets and bony defects of the maxillary first premolars. The patient preferred and chose the second option.
Treatment planning
The key element in orthodontic management of adult patients with periodontal complications is to eliminate or reduce plaque accumulation and gingival inflammation. In this patient, this would imply an emphasis on oral hygiene instruction, appliance construction, and 3-month periodontal check-ups throughout treatment. The extraction of 2 maxillary premolars with more periodontal involvement would be performed only after both teeth were gradually extruded (forced extrusion), with concurrent occlusal trimming to allow gingival and bone apposition and remodeling of the alveolar process. Once leveling and alignment were completed, anterior retraction would be performed with maxillary and mandibular 0.018- × 0.025-inch stainless steel arch wires. After anterior retraction, forced extrusion would also be induced for the maxillary central incisors to achieve better gingival margin levels and create new papillae. After appliance removal, a modified maxillary Hawley retainer and a canine-to-canine mandibular retainer would be installed and bonded, respectively. Reinstructing the patient about oral hygiene measures would be carried out to prevent an increase of the labial gingival recession. Finally, she would be referred to her periodontist.
Methods
Initial periodontal conditions were improved by scaling and root planing before starting the orthodontic treatment. After a 4-month observation period, a careful clinical examination and recording of the periodontal status were performed before orthodontic treatment was initiated. This examination consisted of probing every tooth and checking for mobility, bleeding points, and exudation. Treatment was simultaneously initiated in the maxillary and mandibular arches, with 0.022- × 0.028-inch preadjusted appliances (Elation Esthetic Brackets, DENTSPLY GAC International, Bohemia, NY and Morelli Metal Brackets, Roth prescription, Sorocaba, SP, Brazil) progressively bonded 1 mm more gingivally in the first maxillary premolars than the other brackets to induce extrusion of these teeth during leveling and alignment, with increasingly thicker round nickel-titanium (NiTi) arch wires. As the teeth extruded, they were gradually equilibrated. After 5 months of treatment, leveling and alignment continued with progressively larger round stainless steel arch wires (0.014 to 0.018 inch) with an accentuated and reversed curve of Spee on the maxillary and mandibular arches, respectively. Extrusion of the maxillary first premolars continued with a step-down arch wire bend until normal gingival and bone levels were obtained ( Fig 5 ). Retraction of the anterior maxillary teeth was performed with 0.018- × 0.025-inch stainless steel arch wires with sliding mechanics and without anchorage reinforcement and labial crown torque. Leveling and alignment of the mandibular teeth were obtained following the same wire sequence as the maxillary teeth. Slight proclination of the mandibular anterior teeth was allowed to correct crowding.