Chapter 9
Tooth Replacement in Partially Dentate Older Adults
Aim
As adults are retaining teeth into old age, the requirement for complete replacement dentures will decrease. This chapter aims to describe how decisions can be made regarding tooth replacement in older adults.
Outcome
At the end of this chapter, the practitioner should appreciate that some older adults will seek treatment to replace missing teeth. Fixed and removable prostheses can restore function, appearance and occlusal stability following tooth loss. The practitioner should also understand that poor maintenance of RPDs is associated with high levels of dental disease and that care must be taken to avoid further tooth loss. Preparation of abutments to receive bridge retainers may also endanger the vitality of the teeth and margins of retainers are susceptible to dental caries. The concept of “biological price” should also be understood.
Planning Tooth Replacement
RPDs are one of the most widely used prostheses to replace missing teeth. In this chapter, issues that are particular to the elderly are raised. As was discussed in Chapter 8, it is not always essential to replace missing teeth. Nonetheless, there are a number of clinical situations where some form of prosthesis is required to replace teeth. In older patients, a minimum of twenty teeth is usually required for adequate chewing function. Once the complement of teeth falls below this threshold, chewing ability may diminish to an unsatisfactory level. Should anterior teeth be lost, research indicates that patients are very likely to seek treatment to replace missing teeth. Speech is also affected by loss of teeth, particularly anterior teeth.
Occlusal instability may also occur after loss of teeth. This is manifested in drifting of teeth into adjacent tooth spaces and/or over-eruption of teeth in the opposing arch (Fig 9-1). A further potential consequence of occlusal overloading is drifting of anterior teeth in a buccal direction. This is particularly likely if the anterior teeth have had a significant amount of bone loss.

Fig 9-1 Occlusal instability following the loss of teeth, with drifting of maxillary anterior teeth.
When deciding whether to provide a prosthesis, the clinician must decide if the “biological price” is worth paying. Any prosthesis may potentially compromise oral health – RPDs are associated with increased levels of plaque and fixed prostheses require removal of tooth structure during preparation. If the need to replace teeth is deemed essential, then the biological price may be worth paying.
Fixed or Removable Prostheses?
There are a number of factors to consider when deciding whether to use fixed or removable prostheses to replace missing teeth. The outcome of this decision-making process depends on local and general factors.
Long spans
As a general rule, the risk of failure of fixed bridgework increases when more than two teeth are replaced. This is particularly the case when teeth in the canine or first premolar tooth region are replaced using anterior and premolar teeth. Lateral incisor teeth are regarded as poor-quality retainer teeth as they have short roots and small clinical crowns. A further problem with long-span bridgework is the potential for fracture of the porcelain on porcelain-fused-to-metal bridgework. Precious or semiprecious metal alloy is more flexible than porcelain and consequently when a long span bridge flexes in function, porcelain may fracture. RPDs do not have the same problems and may be more appropriate in longspan situations.
Number of tooth spaces (saddle areas)
As an RPD can replace a number of teeth simultaneously, they are indicated in situations where there are multiple tooth spaces (Fig 9-2). It is possible to use multiple bridges when tooth spaces are small, but this is time consuming and may not be acceptable to the patient.

Fig 9-2 Removable partial dentures can simultaneously replace many teeth, as in this patient.
Soft tissue profile
When teeth have been lost due to trauma, the associated tissues can also be lost. A similar clinical picture can be seen when severe resorption occurs. As well as occlusogingival resorption, bucco-palatal resorption can also occur (Fig 9-3). Replacement of teeth and tissue with a fixed prosthesis can be very difficult, and it may lead to an unsatisfactory aesthetic result (Fig 9-4). The pontic teeth may look very long compared with the retainer teeth. A removable acrylic flange can be constructed to replace resorbed bone and this is placed above the pontics. However, food stagnation is often a problem in such situations. An RPD may be a better option for replacing large amounts of soft tissue, and possibilities should be carefully discussed with the dental technician. The acrylic flange on the denture can be contoured in such a way as to compensate for loss of soft tissue, and a very satisfactory aesthetic result may be achieved (Fig 9-5).
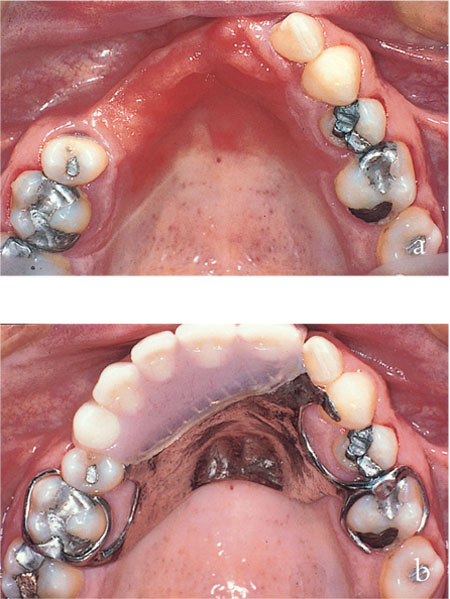
Fig 9-3 Loss of bone as well as teeth occurred following trauma in this patient. Note: (a) the degree of bone loss on the labial aspect of the alveolar ridge; (b) how this is replaced by the removable partial denture. (Courtesy of Dr N Jepson)

Fig 9-4 Poor aesthetic result with conventional bridge-work in a patient with severe alveolar bone loss.

Fig 9-5 Satisfactory cosmetic result achieved with a removable partial denture in a patient with severe alveolar bone loss.
Status of potential abutment teeth
When heavily restored abutment teeth are present, the clinician has to consider what would happen in the event of problems with these teeth. Particular concern arises with teeth that have had endodontic treatment. These are high-risk teeth for failure as bridge abutments and may compromise the entire prosthesis. It may be preferable to use a removable prosthesis if the prognosis of abutment teeth is questionable. If the prognosis is considered favourable, then both fixed and removable prostheses are indicated. Should an RPD be the prosthesis of choice, then heavily restored abutment teeth could have full coverage crown restorations that incorporate features such as rest seats and guide planes (Fig 9-6). The preparation of the teeth in these situations is a little more extensive to allow room for features to be incorporated in the crowns. If surveyed features are planned, then it is essential that design features of the RPD be considered prior to construction of the crowns. A cast of the patient’s teeth should be surveyed and the position of rest, clasps, guide surfaces and connectors planned. This will indicate the ideal position for rest seats, guide planes and undercuts on subsequent full coverage crowns.

Fig 9-6 Milled rest seats and guide surfaces incorporated into full coverage crowns for patient provided with a removable partial denture.
Patient preference
As with any form of dental treatment, the patient’s wishes must be carefully considered. The various treatment options should be discussed in detail with the patient, including advantages and disadvantages. The long-term maintenance requirements must also be carefully discussed. Although a fixed prosthesis may be possible, elderly patients may prefer a less invasive option and choose a removable prosthesis.
Fixed Prostheses in Older Adults: Special Considerations
Should fixed bridgework be chosen, further considerations in older adults include:
-
/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


