Chapter 9
Radiolucencies in the Jaws
Aim
The aim of this chapter is to provide a working knowledge of the more common types of radiolucencies and their differential diagnosis. Some uncommon radiolucencies have also been included to demonstrate the wide variety of lesions that may appear on dental radiographs.
Introduction
Faced with a radiolucency on a dental radiograph, the first questions to answer are:
-
Is it anatomical?
-
Is it artefactual?
The principal anatomical structures that are radiolucent (maxillary sinus, nasal cavity, foramina, etc.) have been described in Chapter 2. It is frequently variations in size or position of these normal structures that cause diagnostic problems.
As far as artefacts are concerned, a “radiolucent” (i.e. “dark”) artefact can result from either overdevelopment (Fig 9-1) or localised exposure to x-rays or light (Fig 9-2).

Fig 9-1 A “radiolucency” caused by a developer splash prior to processing. This patient almost underwent treatment for the “lesion”.
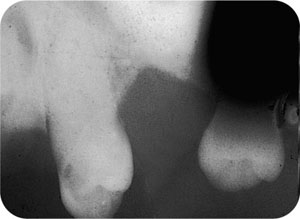
Fig 9-2 A “radiolucency” produced by contamination by daylight from a perforation in the film packet.
If and when these causes of a radiolucency have been excluded, you must consider the pathological causes. Whilst inflammation remains the most common pathological reason for a radiolucency to appear in the jaw (see Chapter 5), there are inevitably many other causes that cannot be covered in their entirety in a book of this size. Table 9-1 provides an overview of this multiplicity of pathology, categorised using the surgical sieve as a template. You are referred to the further reading section at the end of this chapter should you wish to look into this subject in depth.
| Common lesions are in roman type; those in italics are rare. | ||
| Type of Margin Well defined | Ill defined | |
| Anatomical | marrow space; tooth crypt; dental papilla, incisive foramen; maxillary sinus; nasolacrimal duct; sublingual fossa; mental foramen; sub-mandibular fossa; mandibular canal | |
| Developmental/hamartoma | Stafne’s bone cavity; developing odontome; dentinal dysplasia; haemangioma; arterio-venous anomaly | |
| Inflammatory | periapical rarefying osteitis; periapical granuloma; lateral (inflammatory) periodontal cyst | periodontal abscess; periapical rarefying osteitis; infected periapical granuloma; osteomyelitis |
| Cysts | radicular cyst; residual cyst; dentigerous cyst; lateral (developmental) periodontal cyst; keratocyst; nasopalatine cyst; paradental cyst; solitary bone cyst | all cysts if infected |
| Trauma | fractures; alveolar socket seen following traumatic avulsion | fractures if infected |
| Benign tumour | a:odontogenic ameloblastoma; cemento-osseous lesions including: periapical cemental dysplasia, florid osseous dysplasia, cementoossifying fibroma and cementoblastoma; ameloblastic fibroma; odontogenic myxoma b: non odontogenic neurofibroma | primary malignant tumours; langerhans cell histiocytosis; multiple myeloma; metastatic deposits. |
| Malignant tumour | metastatic carcinoma sarcoma | |
| Iatrogenic | surgical (fibrous healing) defect; post-extraction socket | |
| Other | giant cell granuloma; cherubism; aneurysmal bone cyst; fibrous dysplasia | hyperparathyroidism; fibrous dysplasia |
| Artefact | processing errors: developer splash and pooling of developer; air shadows | |
Choice of Radiographs
Periapical radiography is the “first-choice” examination of a small, localised lesion and provides optimal image detail. For larger pathosis, occlusal radiography can be useful in detailing not only the extent of the lesion but also the presence of bony expansion. Panoramic or oblique lateral radiography is needed only in those cases in which the pathosis is more extensive or multiple.
Assessing Radiolucencies in the Jaws
In practice, diagnosis of a radiolucency involves the analysis of certain radiological features, along with the details of the age, sex and racial group of the patient. Using these clinicoradiological features, the practitioner will be able, in the majority of patients, to arrive at a differential diagnosis or, occasionally, a definitive diagnosis. The principle radiographic signs to consider are listed below.
The Site of the Lesion
The probability that a lesion is odontogenic in origin is increased if it is found within alveolar bone and, in the mandible, if it lies above the mandibular canal.
The Shape of the Lesion
A round or ovoid appearance indicates a benign growth pattern such as is typically seen accompanying cysts and benign tumours. In larger cystic lesions, the shape may become more cylindrical as the restraining influence of dense cortical bone limits lateral growth. Malignant and inflammatory lesions have a ragged and very irregular shape, whereas some metabolic/endocrine disorders appear to have no particular shape at all but result in noticeable changes in trabecular pattern.
The Margin and Lumen of the Lesion
The well-defined and corticated margin indicates a slow growing or a static lesion and is seen accompanying the majority of developmental and cystic lesions, and in a number of benign tumours. A well-defined margin reflects an intermediate growth pattern and is seen in some cysts (e.g. solitary bone cyst) and benign lesions (e.g. giant call granuloma). On the other hand, an ill-defined margin demonstrates a rapidly growing lesion, such as occurs in cases of infection and malignancy.
The lumen of the lesion will appear as a single cavity (“unilocular”), multiple cavities (“multilocular”) or can display “pseudolocularity”. In the last-named case, a “scalloped” appearance of the margin can be mistaken for the true multilocular lesion. A scalloped margin is associated with a keratocyst, ameloblastoma and other odontogenic tumours.
The Presence/Absence of Expansion
Most slow-growing benign lesions cause expansion of the cortical plate and concurrent “thinning” of the cortex. Conversely, in more rapidly progressing benign lesions (e.g. giant cell granuloma), perforation of the cortex may accompany expansion. Destruction of the cortical plate is seen in infection, malignancy and any rapidly growing lesion.
Multiplicity of Lesions
Multiple radiolucent lesions are seen in certain cemento-osseous lesions, hyperparathyroidism, multiple myeloma and metastases.
The Presence of a Periosteal Reaction
A periosteal reaction is seen in certain infective/inflammatory lesions (see Chapter 5) and in some malignancies.
The Effect of the Lesion on Other Structures
Slow-growing lesions will displace structures such as teeth, the antral floor and the mandibular canal. More rapidly growing lesions may develop too fast actually to “move” structures. Rapidly growing malignancies destroy supporting alveolar bone giving rise to “floating” teeth.
Resorption of teeth is often seen accompanying a wide variety of pathology (see Table 5-2). Slow-growing lesions, such as odontogenic cysts and benign lesions, will tend to resorb with a clean-cut margin in line with the lesion itself. In more aggressive lesions, typically malignancies and occasionally in severe infection, the pattern of root resorption is more “ragged” and this does not fit with the boundaries of the lesion.
Radiolucencies in the Jaws
Developmental/hamartoma: Stafne’s bone cavity
Stafne’s bone cavity represents a non-palpable depression on the lingual aspect of the mandible and requires no treatment following diagnosis. The aetiology is unknown. It is seen more commonly in middle-aged males. The lesion is asymptomatic and discovered usually as an incidental radiographic finding.
Radiological signs
The lesion presents as a chance radiographic finding. It is a round or an ovoid (< 3cm) uniform radiolucency with a well-defined, usually corticated, margin. Stafne’s bone cavity is non-expansile and is found below the mandibular canal just anterior to the angle of the mandible (Fig 9-3). The location of Stafne’s bone cavity distinguishes it from odontogenic lesions whose origin is within alveolar bone. />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


