9
Case reports
Case 9.1 Class II, division 2 malocclusion
Presentation
Caucasian male, 27 years old with a clear medical history.
No psychological contra-indications to treatment.
Patient’s concerns
Functional:
- Deep and traumatic overbite.
Aesthetic:
- Lower jaw too far back.
- “Collapsed” lower face.
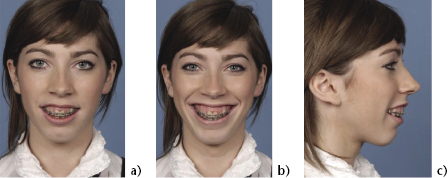
Facial features (Figure 9.1.1)
Antero-posterior:
- Class II skeletal jaw relationship.
- Mandibular retrusion.
- Increased naso-labial angle.
- Progenia.
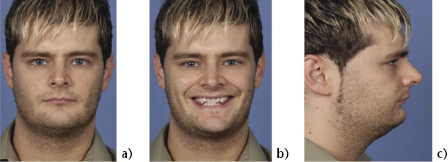
Figure 9.1.1 Frontal view of the face at rest (a) shows the reduced lower anterior face height. A smiling view (b) suggests slightly reduced upper incisor show. The profile view (c) shows a deep labiomental fold accompanied by progenia and the characteristic features of a short facial type.
Vertical:
- Upper incisor show slightly reduced.
- Reduced lower anterior face height.
- Acute labio-mental fold.
- Reduced gonial angle.
- Shallow mandibular plane.
Transverse:
- No obvious facial asymmetry.
Intra-oral features (Figure 9.1.2a)
Dentition:
- Upper incisors retroclined and severely crowded.
- Lower incisors of average inclination and aligned.
- Accentuated lower curve of Spee.
Figure 9.1.2 Intra-orally the upper incisors are retroclined (a), but the presence of severe crowding is favourable for enabling proclination as part of orthodontic decompensation (b).

Occlusion:
- Severe class II, division 2 incisor relationship.
- Overbite 100%, complete and traumatic.
- Overjet minimal.
- Buccal segments greater than a full unit class II bilaterally.
Initial combined plan
Desired soft tissue changes and provisional dento-skeletal movements
Reduce naso-labial angle and increase incisor show:
- Normalise inclination of upper incisors.
- Downgraft anterior maxilla by 2 mm.
Advance the mandible by about 10 mm, improve lip posture and increase LAFH:
- Advance mandible 10 mm (BSSO).
- Correct occlusion to “three-point landing”.
Steepen mandibular and occlusal planes:
- Clockwise rotation.
Achieve optimal vertical proportions and profile balance.
- Vertically augment the chin (genioplasty).
Key objectives of pre-surgical orthodontic treatment
- Procline upper incisors beyond their normal inclination, to compensate for the planned backward maxillary rotation.
- Maintain lower incisor inclination, since backward surgical rotation of the mandible will procline them effectively, relative to the true vertical plane.
- Achieve 10–11 mm overjet (this will allow 10 mm mandibular advancement).
- Maintain lower curve of Spee to allow “three-point landing”.
- Expand maxillary arch to coordinate arches if possible.
Final surgical plan
On completion of pre-surgical orthodontics (Figures 9.1.2b and 9.1.3):
- The upper incisors were at greater than normal inclination (120°).
- The overjet was 11 mm.
- The lower curve of Spee was largely maintained.
- The fit of the occlusion was acceptable, but it was not possible to achieve ideal transverse arch coordination orthodontically.
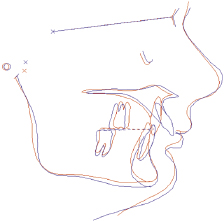
Figure 9.1.3 Superimposition of pre-treatment (red) and pre-surgical (blue) cephalometric tracings shows that the severely retroclined upper incisors were fully decompensated. (Produced using OPAL, British Orthodontic Society).
The surgical plan was finalised, with the aid of model surgery and photo-cephalometric software, as follows:
- Le Fort I anterior downgraft (2 mm) and posterior impaction 2 mm producing some backward (clockwise) rotation of the maxilla. No advancement was possible due to the limitation of mandibular advancement to approximately 10 mm.
- Bilateral sagittal split mandibular advancement 10 mm to three-point landing (Figure 9.1.5a).
- Vertical augmentation genioplasty 3 mm.
Treatment outcome (Figures 9.1.4–9.1.7)
The fact that maxillary advancement was not possible meant that no advancement of the upper lip occured. Some rotation of the maxillo-mandibular complex was acheived with a corresponding steepening of the mandibular plane. The occlusion was largely corrected and dental aesthetics were very satisfactory.
Figure 9.1.4 End of treatment views illustrate that a good improvement in the vertical facial proportions (a) and soft tissue profile (b) were achieved.
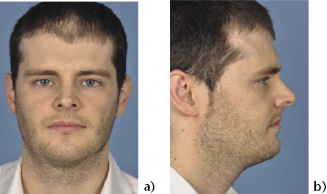
Figure 9.1.5 (a) The “three-point landing” shortly after surgery and (b) the final occlusion, following debond of orthodontic appliances. The lateral open bites were largely closed through a combination of vertical extrusion of the posterior teeth and settling of the overbite.
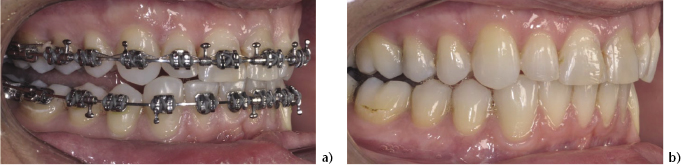
Figure 9.1.6 Cephalometric superimposition of pre-surgical (red) and post-surgical (blue) lateral cephalograms. Both the maxilla and the mandibular body have been rotated downwards and backwards (clockwise), resulting in a steepening of the occlusal and mandibular planes. A vertical augmentation genioplasty has been carried out to achieve optimal vertical proportions. (Produced using OPAL, British Orthodontic Society).
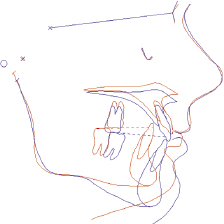
Figure 9.1.7 The vertical position and inclination of the upper incisors are aesthetically pleasing on smiling.

Case 9.2 Vertical maxillary excess
Presentation
Caucasian female, 16 years old with a clear medical history.
No psychological contra-indications to treatment.
Patient’s concerns
Functional:
- Some minor problems chewing.
- Lips do not meet together easily.
Aesthetic:
- Too much gum on show when smiling.
- Lower jaw too far back.
Facial features (Figure 9.2.1)
Antero-posterior:
- Class II skeletal jaw relationship.
- Mild maxillary deficiency.
- Increased naso-labial angle.
- Mandibular deficiency.
Figure 9.2.1 Frontal view of the face at rest (a) and on smiling (b) showing the increased lower anterior face height, the presence of vertical maxillary excess and a short upper lip. The profile view (c) confirms that there is a high FMPA and a downward and backward rotation of the mandible.
Vertical:
- Vertical maxillary excess with excessive gingival display both at rest and on smiling.
- Short upper lip.
- Increased lower anterior face height.
- Steep mandibular plane.
- Retrogenia with obtuse labio-mental fold.
Transverse:
- No obvious asymmetry.
Intra-oral features (prior to orthodontic treatment)
Dentition:
- Upper incisors upright and mildly crowded.
- Lower incisors of average inclination and mildly crowded.
Occlusion:
- Class II, division 1 incisor relationship.
- Overjet 8 mm.
- Buccal segments a full unit class II bilaterally.
Initial combined plan
Desired soft tissue changes and provisional dento-skeletal movements
Reduce gingival display at rest and on smiling.Lengthen upper lip as much as possible.
Increase the prominence of the para-nasal regions by 2–3 mm.
- Anterior maxillary impaction of 5 mm.
- V-Y incision closure.
- Maxillary advancement of 4 mm at Le Fort 1 level.
Advance mandible to optimal occlusion, reduce LAFH and improve lip posture.
- Mandibular autorotation and advancement of 10 mm (which will also require posterior maxillary impaction to achieve positive overbite).
Reduce steepness of occlusal and mandibular planes.
- Anti-clockwise rotation.
Achieve optimal vertical proportions and profile balance.
- Advancement and vertical reduction genioplasty.
Objectives of pre-surgical orthodontic treatment
- Maintain upper incisor inclination to allow for differential posterior impaction of the maxilla.
- Level upper and lower arches.
- Maintain lower incisor inclination. Auto-rotation of the mandible will effectively retrocline the lower incisors relative to vertical.
- Achieve target overjet of 8 mm. This should allow class I incisors to be achieved with approximately 4 mm of maxillary advancement and 10 mm of mandibular advancement plus auto-rotation.
Final surgical plan
On completion of pre-surgical orthodontics (Figure 9.2.2):
- The upper incisor inclinations were still slightly upright.
- The overjet was 8 mm.
- Arch coordination was good.
Figure 9.2.2 Pre-surgical orthodontics produced only minor changes in the incisor inclinations. An overjet of 8 mm was achieved, which enabled the planned amount of mandibular advancement.

The final surgical moves, planned with the aid of model surgery and photo-cephalometric software, were as follows:
- Le Fort I maxillary impaction 5 mm anteriorly and 2 mm posteriorly, with 4 mm advancement.
- Mandibular auto-rotation followed by advancement of 10 mm.
- Genioplasty with 6 mm advancement and 4 mm vertical reduction.
Treatment outcome (Figures 9.2.3–9.2.6)
The degree of gingival display on smiling was greatly reduced, partly due to the maxillary impaction and partly due to upper lip lengthening. The lower anterior face height was reduced significantly but the mandibular plane angle remained steep, because of the short length of the rami. Chin position and lip competence were improved and the occlusion and dental aesthetics were satisfactory.
Figure 9.2.3 The end of treatment frontal view (a) shows improved vertical proportions and lip posture. The profile view (b) shows that there was still a high FMPA, with a degree of profile convexity, but full correction of these features would have been difficult to achieve. Some upper lip lengthening was achieved.

Figure 9.2.4 Superimposition of the pre-surgery (red) and post-surgery (blue) cephalometric tracings confirms that a substantial amount of anterior maxillary impaction and mandibular advancement were achieved. (Produced using OPAL, British Orthodontic Society).
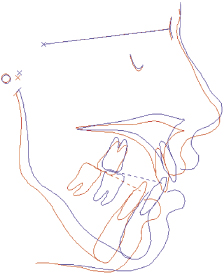
Figure 9.2.5 End of treatment occlusion. A positive overbite and satisfactory inter-digitation were achieved.

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


