Chapter 8
Assessment of Roots and Unerupted Teeth
Aim
The aim of this chapter is to outline the important radiographic features in the assessment of retained roots and unerupted teeth and the appropriate choice of radiographs. Emphasis is placed on those teeth that most commonly fail fully to erupt, mandibular third molars and maxillary canines, and on the assessment of retained roots.
Introduction
It is common for one or more of the permanent teeth to fail fully to erupt. This may be due to insufficient space to accommodate the erupting tooth or because eruption is impeded, for example, by the presence of a supernumerary tooth or a pathological lesion such as a cyst or tumour. More rarely, failure of eruption is seen in systemic conditions, such as cleidocranial dysplasia and Gardner’s Syndrome (see Chapters 6 and 10). Although any tooth may fail to erupt, the commonest ones to do so are mandibular third molars and maxillary canines.
Choice of Radiographs
In the case of a suspected unerupted tooth or retained root, it is important first to undertake a clinical history and examination. The location and number of unerupted teeth determine the need for, and type of, radiographic examination. Where several teeth or roots are thought to be unerupted, especially in more than one quadrant, a DPR is more suitable than several peri-apical views. Selected periapical radiographs can then be taken if the roots or teeth are not clearly shown. In those cases where an unerupted tooth is deeply buried, a periapical radiograph may not show the full extent of the tooth. In such circumstances, a larger film such as an occlusal, oblique lateral or sectional DPR may be more appropriate.
Mandibular Third Molars
Impacted third molars should only be removed provided there is a valid clinical reason for doing so. In the UK, National Guidelines have been produced to assist the clinician with the decision whether third molar removal is required. Most guidelines suggest that wisdom teeth should not be removed unless there is a valid clinical reason for doing so, such as repeated episodes of pericoronitis or unrestorable dental decay of the third molar.
Third molars should always be radiographed prior to removal, even when fully erupted, because of the relative frequency of variable root morphology (Fig 8-1). In addition, it is important to be aware of the proximity of the roots of lower third molars to the mandibular canal. Such a situation may be present even with a fully erupted molar.
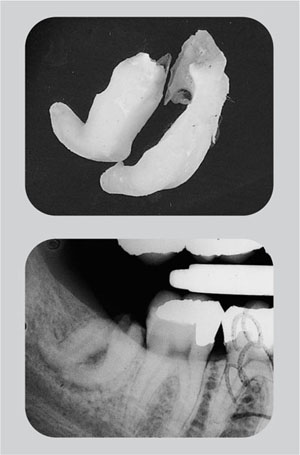
Fig 8-1 No radiograph had been taken prior to the attempted extraction of this lower third molar. Consequently, the operator was unaware of the hooked roots, which resulted in root fracture during extraction.
All unerupted or partly erupted teeth should be assessed in a logical and thorough manner, noting the depth, angulation, root morphology and proximity to other structures such as the mandibular canal and, in the case of an upper third molar, to the floor of the maxillary antrum.
Routine radiographic examination of unerupted third molars is not recommended.
Radiographic Assessment of Mandibular Third Molars
Type and angulation of the impaction
The tooth can be classified as a soft tissue, a tooth, a bone impaction, or a combination thereof. Figs. 8-2 and 8-3 show a soft tissue impaction. The clinical photograph (Fig 8-2) shows the partly erupted lower left third molar to lie vertically and the distal part of the crown to be covered by an operculum. The radiograph (Fig 8-3) confirms the vertical orientation and shows that the crown tooth is not impacted against tooth mesially nor bone, distally. Its only impaction is that of the soft tissue operculum.

Fig 8-2 A partly erupted lower-left third molar.
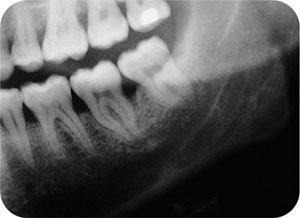
Fig 8-3 Radiograph of the patient shown in Fig 8-2.
The impaction can also be described by the angulation the tooth adopts in relation to the lower second molar. These are:
-
horizontal
-
mesioangular
-
vertical
-
distoangular
-
transverse (rarely).
An example of a transversely impacted third molar is shown in Fig 8-4. Its presence on the bitewing radiograph was an unexpected finding. Fig 8-5 shows a distoangular impaction.

Fig 8-4 Transversely impacted lower third molar. In this situation, a lower true occlusal radiograph would help determine whether the crown is buccally or lingually displaced.
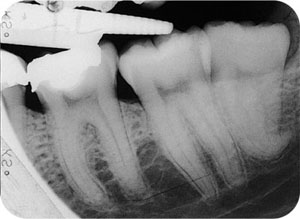
Fig 8-5 A disto-angularly impacted third molar. Note the limited space between it and the second molar tooth and the hook at the apex of the third molar.
The crown
In most cases the presence of caries dictates that the third molar should be removed. When caries is found, it is also important to check the distal aspect of the lower second molar for caries. In many cases, this may be more advanced in the second molar, particularly with mesioangular and horizontal impactions.
Bulbosity of the crown occasionally adds to the difficulty in removing third molars by aggravating the degree of impaction.
The roots
Number
Although most third molars have either one or two roots, the number is variable and there may be as many as four roots. In Fig 8-6, there are three large roots, the mesial root exhibiting hypercementosis. When the roots are large, they are easily identifiable. However, additional roots can be difficult to see, particularly when fine and spindly. In identifying individual roots, it is helpful to trace the outline of the periodontal ligament space. An indistinct apex can mean that two root apices are superimposed upon each other.

Fig 8-6 A mesio-angularly impacted third molar with three large roots. The middle of the three roots is dilacerated in the line of the x-ray beam, as shown by the circular area of increased radiopacity at the apex in the middle of which can be seen the radiolucent dot of the apical foramen. The distal root has a slight mesial curvature, which is in an adverse direction for tooth removal. Hypercementosis also affects the roots of the lower second molar tooth.
Root curvature
Straight roots, or those that are gently curved in a distal direction and follow the path of removal of the tooth, are regarded as favourable. Roots curved in a mesial direction or hooked roots are unfavourable and such teeth may require sectioning in order to deliver the root without fracture. It is important to note whether the individual roots have conflicting paths of withdrawal, as these teeth may also require sectioning. Marked root curvature is shown in Fig 8-7.

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


