(b) 
The 22 was tender to percussion and palpation, and did not respond to thermal (cold) or sensibility testing. The adjacent teeth were asymptomatic and vital.
What did the radiographs (Figure 8.2.2) reveal?
Figure 8.2.2 (a) Pre-operative periapical radiograph revealed a radiolucent area over the mid- to apical-third region of the 22, (b) a second (parallax) view revealed that the radiolucent lesion remained centred, and the gutta-percha point tracked the sinus to its origin.
(a)  (b)
(b) 
The 22 had a radiolucency in the mid- to apical-third of the canal. The radiolucency was symmetrical and elongated in appearance. There was a large periapical radiolucency associated with the tooth (Figure 8.2.2a). A second radiograph of incisor 22 was taken with a distal shift (parallax technique) in direction of the tube head (Figure 8.2.2b); the radiolucency remained in the same position in the canal when compared to the first radiograph. A gutta-percha point was inserted in the sinus prior to taking the second radiograph. This indicated that the source of the infection was from the 22.
When root resorption (external cervical or internal) is suspected, it is desirable to take a cone beam computed tomography (CBCT) scan of the tooth (Figure 8.2.3). This will provide the clinician with three-dimensional views of the tooth. As a result, the severity and true nature of the resorptive lesion (for example perforation of the external root wall) and the restorability of the tooth may be assessed.
Figure 8.2.3 A limited volume cone beam computed tomography scan of the maxillary anterior teeth confirmed the presence of internal root resorption of the 22. (a) Coronal, (b) sagittal, and (c) axial reconstructed images clearly show that resorptive the lesion (yellow arrow) is an extension of the root canal. The resorption lesion has not perforated the root wall. The sagittal slice demonstrates the full extent of the palatal invagination (red arrow). The scan also confirms that the resorptive lesion is treatable.
(a) 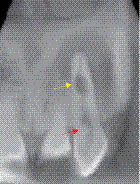 (b)
(b) 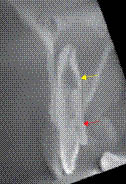 (c)
(c) 
Diagnosis and treatment planning
What was the diagnosis and treatment plan for incisor 22?
The diagnosis was chronic periapical periodontitis with suppuration associated with an infected necrotic pulp and internal root resorption.
Internal root resorption is usually diagnosed as an incidental radiographic finding (Table 8.2.1
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


