Chapter 7
The Contribution of Periodontics to the Correction of Vertical Alveolar Ridge Deficiencies
ALVEOLAR DISTRACTION OSTEOGENESIS SURGERY
History
Alveolar distraction surgery is an application of Ilizarov’s distraction osteogenesis method to the maxillofacial skeleton. Between 1954 and 1971, Gavriel Ilizarov, a Russian orthopedic surgeon, developed a novel surgical approach for reconstruction of skeletal deformities. This involved the use of a mechanical device (the distractor) and the formation of new bone between the bone segments that were gradually separated by incremental traction (Birch and Samchukov 2004). This traction generated tension that stimulated new bone formation parallel to the vector of distraction (Cope and Samchukov 2001, Samchukov 1998). This technique had the added advantage of displacing and preserving the soft tissue with the mobilized bony segment. This is particularly useful in the process of alveolar distraction where the alveolar housing and the surrounding soft tissue are displaced together in a single, simultaneous process (Block 1996, Chin and Toth 1996, McCarthy 1995, Ortiz Mona-sterio 1997).
Indications
- Combined deficiencies in hard and soft tissue not allowing for dental implant placement
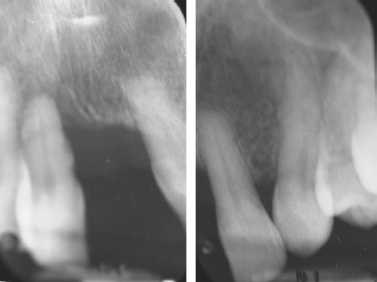
- Vertical alveolar ridge deficiency impairing the placement of a dental implant or fixed partial denture (Figs. 7.1 and 7.2)
Fig. 7.1. Patient presenting with a vertical height defect subsequent to the loss of teeth Nos. 8 and 9.

Fig. 7.2. Tooth No. 8 will be extracted due to severe periodontal disease. Notice the lack of vertical height of the alveolar bone.
- Axial correction of misaligned osseointegrated dental implants or ankylosed teeth
- Orthodontics: Therapy of local open bite
Limitations
- Must have a minimum of 6 mm of residual bone height
- Must have adequate bone width (otherwise block graft necessary before distraction)
- Thin residual bony arch, presenting the risk of fracture
- Patients on bisphosphonates
- Irradiated patients (>40 to 60 Gy)
- Malignancies
- Heavy tobacco use
Advantages (Chiapasco 2004)
- Eliminates the need to harvest bone
- Less operating time
- Distraction histogenesis
- Lower risk of morbidity of the surgical site
- Crestal part of the distracted segment has lower risk of resorption
- Greater vertical bone gain
Armamentarium
- Standard surgical kit, as described in Practical Periodontal Plastic Surgery plus:
- Alveolar Distraction Track Plus Kit (KLS Martin, Jacksonville, FL, USA) and oscillating and sagittal microsaws (KLS Martin, Jacksonville, FL, USA)
Technique for the Anterior Segment
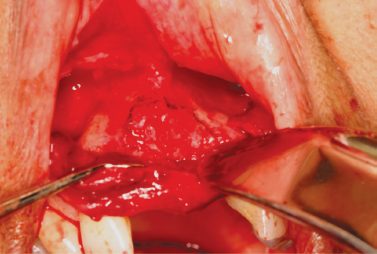
After proper local anesthesia (infiltration with xylocaine 2% with 1:100,000 epinephrine and 1:50,000 epinephrine for hemostasis), an incision is made in the vestibule using a No. 15 blade. The incision is made high enough in the mucosa to allow for proper mobilization of the flap (Fig. 7.3). The incision may be done in two steps: incision of the mucosal layer first, then incision of the connective tissue, muscles, and periosteum. Keep the blade oriented toward the alveolar bone. The incision has to be long enough to allow for easy blunt dissection with a periosteal elevator.
Fig. 7.3. The incision is high up in the vestibule to allow for flap mobilization and access.

The role of the elevator is to now reflect the flap all the way up to the alveolar crest of the edentulous site but not beyond (Figs. 7.4 and 7.5). It is critical to leave the palatal or lingual periosteum attached to the bone, because it will be the only source of vascularization of the bony fragment during the distraction process. Once the bony area is exposed, it is useful to draw a picture of the segment to be distracted on the bone using a sterile No. 2 pencil (Fig. 7.6). The base of the bony segment should be wider at the crest than apically (Fig. 7.7) to allow for unimpaired sliding movement during the traction process. Also at this point, it is important to remember that the distracted segment should be no shorter than 5 mm.
Fig. 7.4. The full-thickness flap is reflected using a periosteal elevator.
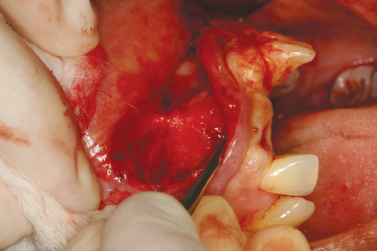
Fig. 7.5. Reflection stops at the alveolar crest.
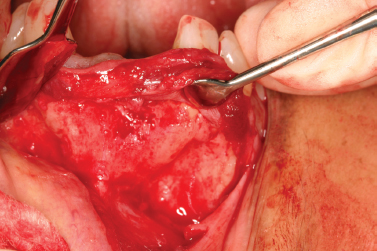
Fig. 7.6. The segment to be distracted is delineated with a sterile No. 2 pencil.
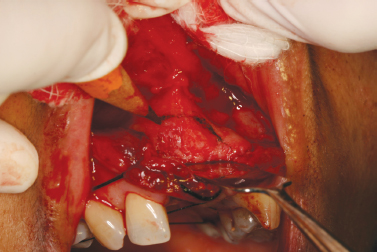
Fig. 7.7. The segment to be cut is drawn on the bone. Notice the divergence of the cuts that will allow for free movement of the segment.
Once the segment is visualized, it is time to adapt the distractor to fit the clinical picture. This is the most time-consuming part of the operation, because one has to adapt (cut) and bend the upper and lower arms of the distractor to fit the underlying bone architecture, while preserving the proper direction of the vector (Figs. 7.8 to 7.10). Distractors are available in 6-, 9-, 12-, and 15-mm lengths. After predrilling one hole for each arm while holding the distractor in place, the sagittal saw (set at 20,000 RPM) is used to cut the bone (Fig. 7.11). It is better not to do a through-and-through cut at the beginning but to get as close as possible to the palatal/lingual bony plate (Fig. 7.12). Also, the orientation of the saw should always be kept slightly angled toward the alveolar crest; this will prevent invasion of anatomical structures (i.e., the nasal spine, the nasal cavity, or the genial tubercules).
Fig. 7.8. The distractor is modified to fit the clinical picture.

Fig. 7.9. The distractor is placed, verifying the correct direction of the distraction vector.
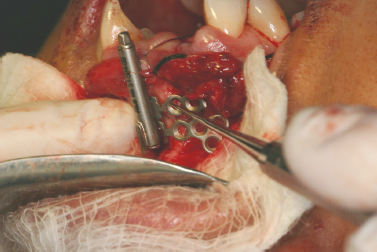
Fig. 7.10. One hole in each arm o/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


